

Bilirubin is a yellowish substance produced during the normal process of breaking down old red blood cells, which must be processed by the liver and excreted from the body to prevent health complications. In a healthy biological system, the liver acts as a filter to remove this pigment from the bloodstream, eventually passing it out of the body through bile into the digestive tract. However, if the liver is damaged, or if there is an obstruction preventing the bile from draining, bilirubin can build up in the blood. When levels become significantly elevated, the pigment begins to settle into the tissues, leading to the yellow discoloration of the skin and eyes known as jaundice. In the United Kingdom, healthcare professionals use bilirubin levels as a key indicator of liver, gallbladder, and blood health. Understanding the life cycle of this pigment is essential for recognising how metabolic imbalances or physical obstructions can manifest as visible changes in the body.
What We’ll Discuss in This Article
- The biological origin of bilirubin during red blood cell breakdown.
- The liver’s role in conjugating bilirubin for safe excretion.
- The chemical transition from fat-soluble to water-soluble bilirubin.
- How a buildup of this pigment causes the physical signs of jaundice.
- Common causes for the interruption of the bilirubin metabolic pathway.
- The importance of clinical monitoring and blood tests in the UK.
The Biological Production of Bilirubin
Bilirubin is a natural byproduct formed when the body recycles aged red blood cells that have reached the end of their typical lifespan. These cells contain haemoglobin, the protein responsible for carrying oxygen, which is broken down into various components, including a substance called heme. The body then converts heme into a yellowish pigment known as unconjugated or “indirect” bilirubin. The NHS states that jaundice is caused by the build-up of bilirubin in the blood, which often occurs if the liver is damaged or there is a problem with the bile ducts.
At this initial stage, unconjugated bilirubin is fat-soluble, meaning it cannot be dissolved in water or excreted easily by the kidneys. It must be transported through the bloodstream, bound to a protein called albumin, until it reaches the liver. Under normal circumstances, this is a continuous and efficient recycling process. Jaundice only begins to manifest when the volume of bilirubin produced exceeds the liver’s ability to process it or when the liver’s processing machinery is compromised by disease.
The Liver’s Role in Processing and Conjugation
The liver performs the vital task of “conjugating” bilirubin, a chemical transformation that makes the pigment water-soluble and allows it to be safely moved out of the body. Once the unconjugated bilirubin enters the liver cells, an enzyme attaches a sugar molecule to it, turning it into conjugated or “direct” bilirubin. This conjugated form can now be dissolved in bile, the digestive fluid produced by the liver.
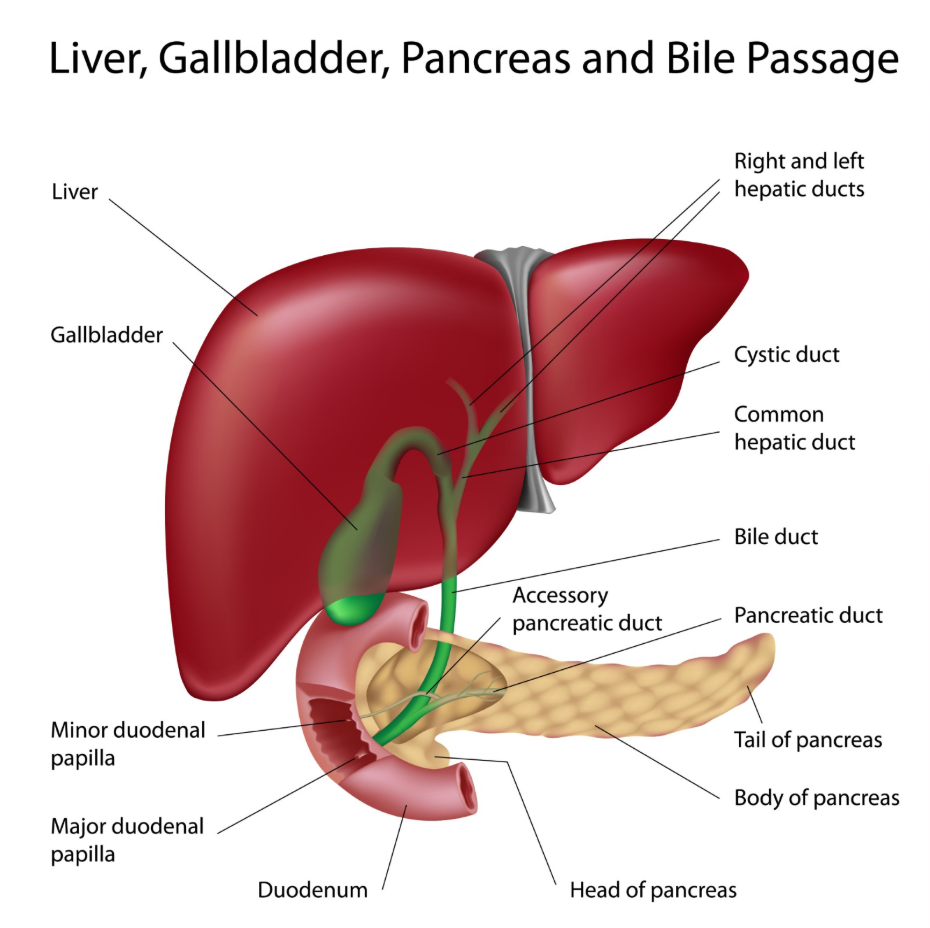
After conjugation, the liver pumps the bilirubin into the small drainage tubes known as bile ducts. These ducts lead to the gallbladder for storage or directly into the small intestine. In the gut, bacteria further break down the bilirubin into substances that give stools their characteristic brown colour. If the liver is healthy and the bile ducts are clear, very little bilirubin remains in the blood. However, if the liver is scarred or inflamed, it may struggle to conjugate the pigment, or it may be unable to pump the conjugated bilirubin into the ducts, leading to a backup into the circulatory system.
How Bilirubin Causes Jaundice
Jaundice occurs when the concentration of bilirubin in the blood rises to a level where it begins to leak out of the blood vessels and deposit into the skin and mucous membranes. Bilirubin has a high affinity for elastic tissue, which is found in high concentrations in the whites of the eyes and the skin. When the pigment binds to these tissues, it creates the yellow hue that is the hallmark of jaundice.

The whites of the eyes, or sclera, are often the first place jaundice becomes visible because they are naturally white and contain high levels of elastin, making even small amounts of the yellow pigment easy to spot. As bilirubin levels continue to climb, the yellowing spreads to the face, torso, and eventually the limbs. This physical change is not a disease in itself but a visible signal that the body’s filtration and excretion system for bilirubin is currently failing to keep pace with production or drainage requirements.
Interruption of the Excretion Pathway
There are several points where the processing and excretion of bilirubin can be interrupted, each leading to different clinical scenarios of jaundice. Clinicians in the UK often categorise these based on where the problem occurs: before the liver, inside the liver, or after the liver in the drainage system.
| Category | Location of Issue | Common Mechanism |
| Pre-hepatic | Bloodstream | Excessive breakdown of red blood cells (haemolysis). |
| Intra-hepatic | Liver Tissue | Liver cell damage from infection, toxins, or scarring. |
| Post-hepatic | Bile Ducts | Obstruction by gallstones, inflammation, or tumours. |
In post-hepatic cases, also known as obstructive jaundice, the liver has successfully conjugated the bilirubin, but a physical blockage prevents it from entering the intestine. This can cause the urine to turn dark because the water-soluble conjugated bilirubin is filtered out by the kidneys instead. Simultaneously, the stools may become pale or clay-coloured because the pigment that normally gives them their colour is unable to reach the digestive tract. According to the GOV.UK health pages, identifying whether jaundice is obstructive is a clinical priority to ensure that the cause of the blockage is managed to prevent further organ damage.
Clinical Monitoring of Bilirubin Levels
In the UK, the measurement of total, conjugated, and unconjugated bilirubin through blood tests is a standard part of assessing liver and gallbladder health. These tests help healthcare professionals determine the likely source of the jaundice by looking at which type of bilirubin is most elevated. If unconjugated levels are high, it may point toward a blood-related issue; if conjugated levels are high, it suggests a problem with the liver’s ability to excrete the pigment or a blockage in the bile ducts.
NICE clinical guidelines for liver disease management emphasise that bilirubin levels must be interpreted alongside other liver enzyme tests to provide an accurate picture of the organ’s functional capacity. Regular monitoring allows for the tracking of disease progression or the success of treatments aimed at clearing obstructions or reducing liver inflammation. Because the liver is involved in so many metabolic pathways, an elevated bilirubin level is often the first clear signal that the body’s internal chemistry requires professional medical investigation.
Conclusion
Bilirubin is a natural pigment derived from red blood cell recycling that must be processed by the liver and excreted through bile to maintain health. Jaundice occurs when bilirubin levels in the blood rise due to excessive production, liver damage, or bile duct obstruction, leading the pigment to deposit in the skin and eyes. While the yellowing is the most visible symptom, the underlying cause determines the clinical significance and the required management plan. Routine monitoring of bilirubin levels through the NHS provides an essential window into the functional status of the liver and biliary system. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does high bilirubin always mean I have liver disease?
No, high bilirubin can also be caused by blood conditions that break down red blood cells too quickly or by blockages like gallstones.
Why does bilirubin make my urine turn dark?
If conjugated bilirubin builds up in the blood because it cannot drain into the gut, the kidneys filter it out, which turns urine a tea-like colour.
Can a healthy person have high bilirubin?
Yes, a common genetic condition called Gilbert’s syndrome can cause mild, harmless fluctuations in bilirubin levels without liver damage.
Is bilirubin toxic?
In adults, mildly elevated levels are usually just a symptom, but very high levels can occasionally cause itching or malaise; in newborns, very high levels require urgent care.
How long does it take for bilirubin levels to drop?
This depends on the cause; once an obstruction is cleared or liver inflammation subsides, levels can begin to fall within a few days.
Can diet lower my bilirubin levels?
Diet alone cannot lower bilirubin, but a healthy lifestyle supports the liver, and avoiding alcohol reduces the toxic stress on the organ.
Why are my stools pale when my bilirubin is high?
If a blockage prevents bilirubin from reaching your intestines, the stools lose the pigment that normally turns them brown.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding bilirubin and jaundice, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
