


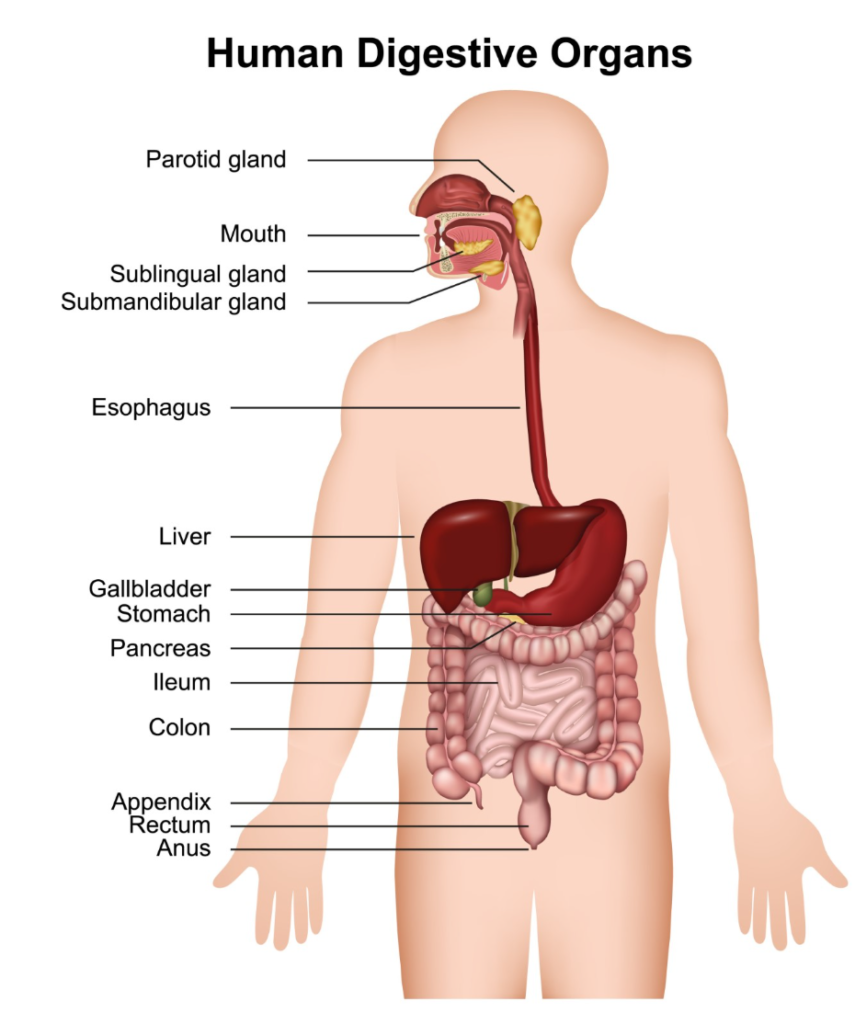
Pancreatitis is a clinical condition defined by the inflammation of the pancreas, a specialised glandular organ situated deep within the upper abdomen, positioned behind the stomach and in close proximity to the first part of the small intestine. In the United Kingdom, understanding the specific anatomy of the pancreas is essential for patients to comprehend how inflammation can disrupt vital bodily functions, including digestion and blood sugar regulation. The pancreas is divided into distinct anatomical regions, and while pancreatitis can begin in one specific section, the inflammatory process often spreads to affect the entire organ and potentially the surrounding tissues. Because the pancreas is located near several major blood vessels and other digestive organs, such as the gallbladder and liver, inflammation can have widespread implications for a patient’s health. UK healthcare professionals utilise advanced imaging and clinical assessments to determine the extent of the inflammation and to monitor for complications. By adhering to the evidence-based frameworks provided by the NHS and the National Institute for Health and Care Excellence, medical teams can provide targeted care that addresses the specific anatomical and functional challenges posed by this serious condition.
What We’ll Discuss in This Article
- The anatomical divisions of the pancreas: head, body, and tail
- How inflammation typically spreads through the pancreatic tissue
- The role of the pancreatic duct in the development of pancreatitis
- The impact of inflammation on the endocrine and exocrine cells
- How proximity to other organs influences the severity of the condition
- The biological consequences of tissue damage within the organ
- NHS methods for assessing the extent of pancreatic involvement
Pancreatitis affects the pancreas itself, which is divided into the head, body, and tail, though the inflammation often spreads across the entire organ
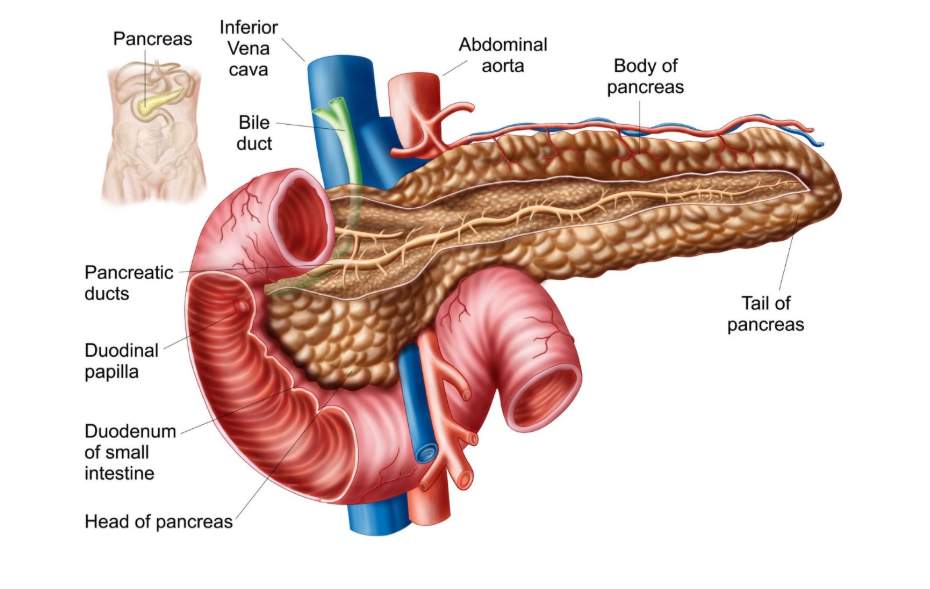
The pancreas is an elongated organ with a complex structure that serves dual roles in the human body. Pancreatitis is inflammation of the pancreas, a small organ located behind the stomach that helps with digestion. Anatomically, the “head” of the pancreas is the widest part and lies in the curve of the duodenum, the “body” extends horizontally behind the stomach, and the “tail” is the narrow end that reaches toward the spleen. While an inflammatory event, such as a blockage caused by a gallstone, may originate near the head where the pancreatic duct enters the intestine, the resulting chemical reaction of prematurely activated enzymes often causes swelling and damage throughout the body and tail of the organ as well.
The involvement of the pancreatic duct
The pancreatic duct is a central channel that runs the length of the organ, and it is frequently the starting point for the pressures that lead to pancreatitis. This duct carries digestive juices to the small intestine; however, if it becomes obstructed by a stone or narrowed by inflammation, these potent fluids are trapped. The most common cause of acute pancreatitis is gallstones, which can block the opening of the pancreatic duct. When the duct is blocked, the internal pressure rises, causing the enzymes to leak into the surrounding pancreatic tissue. This initiates a process of auto digestion, where the organ’s own secretions begin to break down its cellular structure, leading to the intense pain and systemic inflammation characteristic of an acute episode.
Impact on exocrine and endocrine functions
Pancreatitis affects the two primary types of functional tissue within the organ: the acinar cells and the islets of Langerhans. The acinar cells are part of the exocrine system and are responsible for producing digestive enzymes; these are usually the first cells to be damaged during an inflammatory flare. The islets of Langerhans make up the endocrine system and produce hormones like insulin and glucagon. In severe or chronic cases of pancreatitis, the damage can extend to these endocrine clusters. Chronic pancreatitis is where the pancreas has been permanently damaged from inflammation over many years, which can lead to diabetes if the insulin producing cells are destroyed. This explains why long term pancreatic health is so closely tied to a patient’s ability to regulate their blood sugar levels.
Proximity to surrounding structures
Because of its deep location in the retroperitoneum, inflammation of the pancreas can affect several neighbouring structures and organs. The head of the pancreas is in intimate contact with the common bile duct; therefore, swelling in this region can compress the duct and lead to jaundice. Furthermore, the pancreas sits directly in front of the portal vein and the superior mesenteric artery, which are major blood vessels. In severe acute pancreatitis, the inflammatory fluids and enzymes can leak out of the pancreas and irritate the lining of the abdominal cavity or cause fluid collections near the stomach and spleen. UK clinicians monitor these areas closely during hospital admission to ensure that the inflammation does not lead to secondary complications in these vital adjacent structures.
Comparison of Pancreatic Regions and Potential Involvement
| Region | Anatomical Position | Clinical Significance in Pancreatitis |
| Head | Nestled in the duodenum | Most common site for ductal blockages |
| Body | Behind the stomach | Often shows significant swelling and fluid buildup |
| Tail | Near the spleen | Damage here can affect the majority of insulin cells |
| Pancreatic Duct | Central channel | Blockage here is the primary trigger for enzymes |
Tissue damage and necrosis
When pancreatitis is severe, the lack of blood flow to certain parts of the organ can cause the tissue to die, a process known as necrosis. Necrosis can affect any part of the pancreas, but it is often seen in the body or tail following a severe acute attack. Necrotic tissue is highly susceptible to infection, which is a life threatening complication. In the United Kingdom, specialists use contrast enhanced CT scans to identify which parts of the pancreas are receiving adequate blood supply and which have been compromised by the inflammatory process. According to the National Institute for Health and Care Excellence, patients with suspected severe pancreatitis should be monitored for signs of organ failure or infected necrosis. This detailed anatomical assessment is crucial for determining if a patient requires surgical intervention or intensive supportive care.
Functional recovery and the tail of the pancreas
The tail of the pancreas contains a higher concentration of the islet cells that produce insulin compared to the head. Consequently, if an inflammatory episode primarily affects the tail, the risk of developing “Type 3c” diabetes is significantly higher. During recovery from pancreatitis in the UK, healthcare teams assess the functional capacity of the remaining healthy tissue. While the pancreas has some ability to recover from minor acute inflammation, repeated episodes or extensive necrosis can lead to a permanent reduction in organ size and function. Long term management often focuses on supporting the remaining parts of the pancreas through dietary changes and enzyme replacement therapy to compensate for the tissue that has been lost or permanently scarred.
Conclusion
Pancreatitis affects the entire pancreas, including its head, body, and tail, as well as the central ductal system. While inflammation may begin in one region due to a blockage, it frequently spreads to involve both the enzyme producing and hormone producing tissues. The proximity of the pancreas to major blood vessels and the small intestine means that the effects of inflammation are often felt beyond the organ itself. Following NHS and NICE guidelines ensures that the extent of the damage is accurately assessed and managed. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can you live without a pancreas if it is completely damaged?
Yes, it is possible to live without a pancreas, but you would require lifelong insulin injections and enzyme replacement therapy to digest food.
Does pancreatitis always affect the gallbladder too?
Not directly, but gallstones are a leading cause of pancreatitis, and the two organs share a drainage pathway into the small intestine.
Why does the pain of pancreatitis often go through to the back?
The pancreas is located deep in the abdomen, close to the spine and major nerve plexuses, which causes the pain to radiate backward.
Can only part of the pancreas be inflamed?
In some early or mild cases, inflammation might be localised, but the nature of digestive enzymes means it usually spreads across the whole organ quickly.
Does the tail of the pancreas do something different than the head?
The tail has a higher density of insulin producing cells, while the head is more involved with the drainage of digestive enzymes into the gut.
What happens if the inflammation affects the duodenum?
Severe swelling in the head of the pancreas can sometimes narrow the duodenum, making it difficult for food to pass through the stomach.
Is the spleen affected by pancreatitis?
Because the tail of the pancreas sits very close to the spleen, inflammation or fluid collections can sometimes cause issues with the splenic blood vessels
Authority Snapshot (E-E-A-T Block)
This article was developed by the Medical Content Team to provide clear education on the anatomy and clinical impact of pancreatic inflammation. The content has been reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in general surgery and emergency medicine, to ensure absolute alignment with NHS and NICE clinical guidance. Our purpose is to help the public understand the physical reality of this condition through factual and restrained reporting.


