

Viral hepatitis leads to cirrhosis and liver cancer through a process of chronic inflammation where the body’s immune response to the virus repeatedly damages liver cells over many years. When the liver is constantly injured by a persistent viral infection, such as Hepatitis B or Hepatitis C, it attempts to heal itself by creating fibrous scar tissue. This ongoing cycle of cell death and repair eventually replaces healthy, functional liver tissue with extensive scarring, which is the definition of cirrhosis. Furthermore, the rapid cell turnover and genetic instability caused by the virus significantly increase the likelihood of mutations that can trigger the development of primary liver cancer. In the United Kingdom, managing viral hepatitis through early detection and antiviral therapy is the primary method for preventing these life-threatening complications.
What We’ll Discuss in This Article
- The biological transition from chronic inflammation to liver scarring.
- How the immune system’s response to the virus damages healthy liver cells.
- The physical progression from early-stage fibrosis to advanced cirrhosis.
- The link between rapid cell regeneration and cancerous mutations.
- Why Hepatitis B and C pose a higher risk for hepatocellular carcinoma.
- Methods used in the UK for monitoring liver health and cancer risk.
From Infection to Chronic Inflammation
Viral hepatitis causes long-term liver damage primarily because the virus remains inside the liver cells, triggering a persistent immune response that never fully resolves. While the virus itself can damage the cells, much of the injury is caused by the body’s own white blood cells attacking the infected hepatocytes. The NHS states that if hepatitis is not treated, it can lead to scarring of the liver, known as cirrhosis, and increases the risk of developing liver cancer.
This state of chronic inflammation means the liver is under constant stress. Unlike acute hepatitis, which may resolve in a few weeks, chronic infections can last for decades. During this time, the liver is unable to perform its usual metabolic and filtration duties efficiently because its resources are diverted toward managing the inflammatory environment. This persistent inflammation provides the biological foundation for the development of more severe structural damage.
The Development of Liver Fibrosis and Cirrhosis
Cirrhosis develops when the liver’s natural healing process is overwhelmed by continuous viral injury, leading to the excessive accumulation of fibrous scar tissue. When liver cells are destroyed by the immune system, the liver produces collagen to bridge the gaps. Initially, this scarring is mild and known as fibrosis, but as the viral infection persists, the scar tissue becomes more dense and widespread.
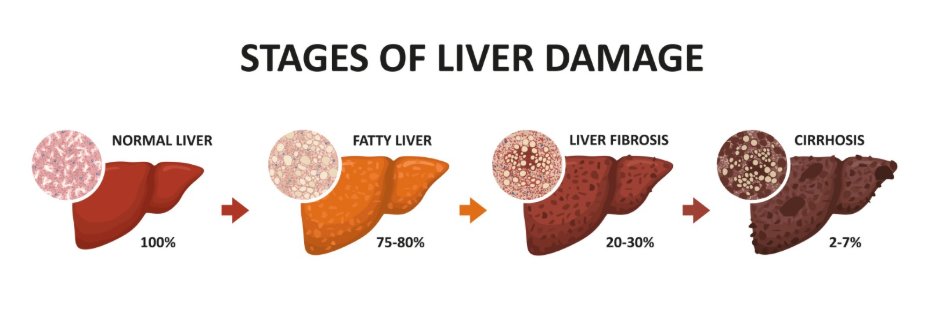
Over time, these bands of scar tissue begin to encircle nodules of regenerating liver cells, completely distorting the organ’s internal architecture. This advanced stage is called cirrhosis. The hard, scarred tissue obstructs blood flow through the liver, which can lead to high pressure in the portal vein and significantly impair the liver’s ability to produce essential proteins or detoxify the blood. In the UK, clinicians use non-invasive tests to measure liver stiffness and determine how far this scarring has progressed.
Genetic Instability and Cancerous Mutations
The progression from cirrhosis to liver cancer is driven by the genetic errors that occur when liver cells are forced to divide at an abnormally high rate. In a liver affected by chronic hepatitis, the body is constantly trying to replace dead cells with new ones. This rapid cell turnover increases the mathematical probability of a mutation occurring in the DNA during the replication process.
When mutations occur in specific genes that control cell growth or suppress tumours, the affected cell may begin to multiply uncontrollably, forming a malignant tumour. This is the most common way that hepatocellular carcinoma, the primary form of liver cancer, begins. The risk is highest once cirrhosis is established, as the scarred environment itself promotes the survival of abnormal cells and suppresses the immune system’s ability to clear them.
The Specific Roles of Hepatitis B and C
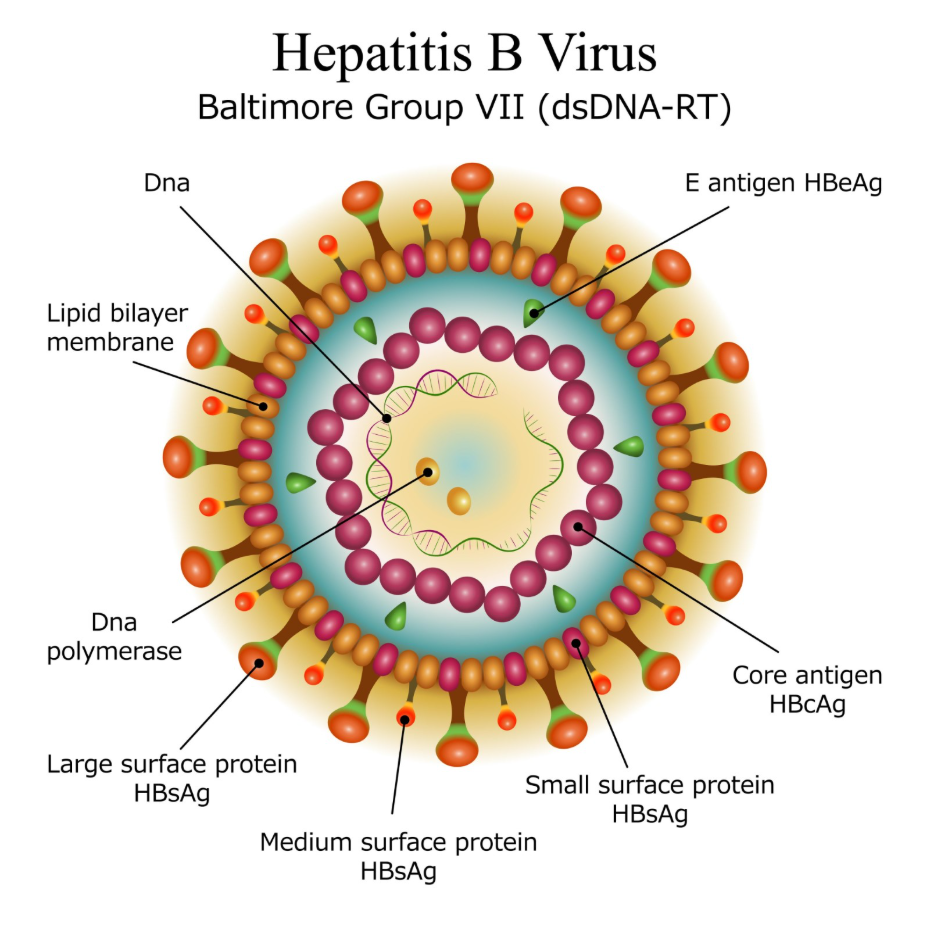
While both Hepatitis B and Hepatitis C lead to cirrhosis, they have slightly different biological mechanisms for increasing cancer risk. Hepatitis C primarily causes cancer through the long-term cycle of inflammation and cirrhosis. In contrast, the Hepatitis B virus can integrate its own genetic material into the DNA of the host liver cell, which can directly trigger cancerous changes even before significant cirrhosis has developed.
| Feature | Hepatitis B | Hepatitis C |
| Transmission | Blood and bodily fluids | Primarily blood-to-blood |
| Primary Cancer Driver | Genetic integration and inflammation | Chronic inflammation and cirrhosis |
| UK Prevention | Vaccination and antivirals | Curative antiviral tablets |
| Cancer Risk | Can occur without cirrhosis | Mostly occurs after cirrhosis |
NICE clinical guidelines emphasise that individuals with chronic hepatitis B or C should be monitored regularly for liver cancer because the risk persists even if the virus is currently well-controlled. This surveillance is vital for catching tumours early when they are most treatable.
Clinical Monitoring and Surveillance in the UK
In the United Kingdom, patients with chronic viral hepatitis who have developed significant scarring are placed on a formal surveillance pathway. This typically involves an ultrasound scan of the liver every six months to check for the development of new nodules or tumours. Clinicians may also use blood tests to measure specific markers that are often elevated in the presence of liver cancer cells.
The goal of this monitoring is to identify changes at a stage where curative treatments, such as surgery or ablation, are still possible. The GOV.UK health pages indicate that early detection through regular screening is the most effective way to improve the long-term survival of patients with cirrhosis caused by viral hepatitis. Adhering to these six-monthly appointments is a critical part of managing the long-term risks associated with a chronic viral infection.
Conclusion
Viral hepatitis leads to cirrhosis and liver cancer by triggering a persistent cycle of inflammation, cell death, and disordered repair. The resulting scar tissue permanently alters the liver’s function, while the rapid cell regeneration creates a high-risk environment for the genetic mutations that cause tumours. Consistent medical care, antiviral treatment, and regular clinical surveillance are essential for managing these risks and protecting liver health. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does everyone with Hepatitis C eventually get cirrhosis?
No, many people who receive early treatment with modern antivirals can clear the virus before significant scarring occurs.
Can liver cancer develop if I don’t have cirrhosis?
It is possible, particularly with Hepatitis B, but the vast majority of liver cancer cases occur in people who already have cirrhosis.
How long does it take for cirrhosis to develop from hepatitis?
It is usually a slow process that takes between twenty and thirty years of chronic infection.
Will treating the virus reverse the scarring on my liver?
Treating the virus stops further damage and may allow early-stage scarring to improve, but advanced cirrhosis is generally permanent.
Why is Hepatitis B more likely to cause cancer in younger people?
The virus can integrate into the DNA early in life, providing more time for mutations to accumulate as the person grows.
Can a healthy lifestyle stop hepatitis from becoming cancer?
A healthy lifestyle and avoiding alcohol can slow the progression of liver damage, but medical treatment for the virus is the most important factor.
What are the early signs that hepatitis is turning into cancer?
There are often no symptoms in the early stages, which is why regular ultrasound scans are essential for those at high risk.
Authority Snapshot (E-E-A-T)
This article provides medically factual health information regarding the progression of viral hepatitis, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in internal medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
