

A blocked bile duct leads to jaundice by creating a physical obstruction that prevents the normal flow of bile from the liver into the digestive tract, causing a yellow pigment called bilirubin to back up into the bloodstream. In a healthy biological system, the liver filters bilirubin from the blood and excretes it as a major component of bile. When the network of drainage tubes, known as the biliary tree, is restricted by stones or inflammation, this excretion pathway is severed. This specific type of jaundice is medically referred to as obstructive or post-hepatic jaundice. Because the liver has already processed the bilirubin, the excess pigment in the blood is water-soluble, which leads to distinct changes in the appearance of bodily waste. In the United Kingdom, identifying a biliary blockage is a clinical priority because it indicates a structural “plumbing” issue that requires intervention to prevent further complications such as infection or liver inflammation. Understanding the anatomy and function of the bile ducts is essential for recognising why a localised blockage results in the systemic symptom of yellowing skin and eyes.
What We’ll Discuss in This Article
- The biological journey of bilirubin from the liver to the intestines.
- Common causes of biliary obstruction, including gallstones and tumours.
- The mechanism of “backflow” where bile enters the circulatory system.
- Distinct physical indicators such as dark urine and pale, clay-coloured stools.
- Clinical pathways in the UK for diagnosing and resolving a blocked duct.
- Potential complications of untreated biliary obstructions like cholangitis.
The Normal Excretion Pathway of Bilirubin
To understand how a blockage causes jaundice, it is necessary to first examine the liver’s role in processing bilirubin and moving it through the bile ducts. Bilirubin is a yellow-orange pigment produced during the breakdown of old red blood cells. The NHS explains that jaundice is caused by the build-up of bilirubin in the blood, which can happen if there is a problem with the bile ducts that prevents it from leaving the body.
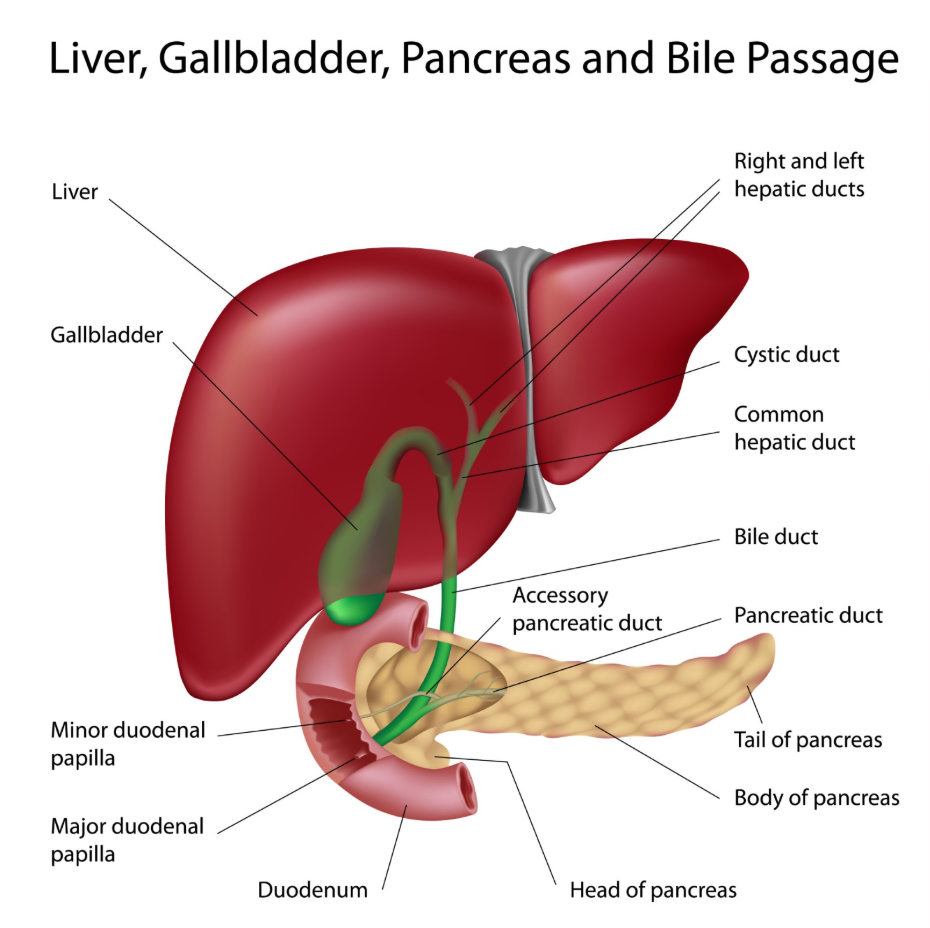
The liver cells take up this pigment and “conjugate” it, making it water-soluble. This processed bilirubin is then secreted into tiny channels that merge to form the common bile duct. Under normal conditions, this duct carries bile into the small intestine to assist with the digestion of fats. Once in the gut, bacteria convert the bilirubin into stercobilin, which provides the brown colour of stools. If the ducts are clear, very little of this processed bilirubin remains in the blood, and the body’s metabolic waste cycle remains balanced.
Mechanisms of Physical Biliary Obstruction
A blocked bile duct occurs when a physical mass or inflammation narrows the passage of the common bile duct, preventing the exit of bile. This is an obstructive process where the liver continues to produce bile, but the fluid has no exit route. As the pressure within the biliary tree increases, the conjugated bilirubin is forced out of the ducts and back into the liver’s blood vessels.
| Cause of Blockage | Description | Clinical Significance |
| Gallstones | Solidified bile deposits that migrate from the gallbladder. | Most common cause of acute blockage. |
| Bile Duct Cancers | Tumours growing within the lining of the ducts. | Requires urgent specialist oncology review. |
| Pancreatic Tumours | Growths at the head of the pancreas pressing on the duct. | Often presents with “painless” jaundice. |
| Biliary Strictures | Narrowing caused by inflammation or previous surgery. | Leads to chronic or intermittent jaundice. |
In the United Kingdom, gallstones are the most frequent trigger for this type of jaundice. When a stone gets stuck, the resulting pressure change is immediate. Unlike liver disease, where the cells themselves are failing, obstructive jaundice is a mechanical failure. The liver cells are often initially healthy and continue to conjugate bilirubin, but they cannot overcome the physical cap on the drainage system.
Systemic Effects: Dark Urine and Pale Stools
The backflow of bilirubin into the blood during a blockage creates a unique set of symptoms that affect the colour of urine and stools. Because the bilirubin involved in a blockage has already been processed by the liver, it is water-soluble. This allows the kidneys to filter the excess pigment out of the blood and into the urine, which turns a dark orange or tea-like colour.
Simultaneously, the absence of bile in the intestines means that no pigment reaches the digestive tract. This results in stools that appear pale, grey, or clay-coloured. NICE clinical guidelines for the management of biliary disease highlight that the combination of jaundice, dark urine, and pale stools is a hallmark indicator of an obstructive process. Additionally, the lack of bile in the gut prevents the proper absorption of fats, which can lead to greasy, foul-smelling stools (steatorrhoea). These visible changes in waste are critical clues that help UK clinicians differentiate between a “plumbing” issue and a blood or liver cell disorder.
Managing the Risks of Biliary Infection
A major concern with a blocked bile duct is the risk of stagnant bile becoming infected, a condition known as ascending cholangitis. When bile is not flowing, it creates a fertile environment for bacteria to multiply. If an infection develops, it can quickly spread to the bloodstream, leading to sepsis. In the UK healthcare system, jaundice accompanied by fever and right-sided abdominal pain is treated as a clinical emergency.
To manage these risks, clinicians prioritise the relief of the obstruction. While antibiotics can treat the infection, the underlying blockage must be cleared to prevent recurrence. This integrated approach ensures that the liver is not subjected to prolonged pressure or systemic infection, both of which can lead to secondary liver damage. Regular monitoring of inflammatory markers in the blood is a standard part of care for anyone with suspected biliary obstruction.
Clinical Investigation and Resolution in the UK
In the United Kingdom, the investigation of a suspected blocked bile duct involves imaging to locate the obstruction and blood tests to confirm the obstructive pattern. Ultrasound is typically the first-line imaging tool used to check if the bile ducts are dilated or widened. If a blockage is suspected, a more detailed scan such as an MRI (MRCP) or a specialised procedure called an ERCP may be used.
During an ERCP, a specialist uses an endoscope to reach the opening of the bile duct in the small intestine. They can then use X-rays to see the blockage and often remove a gallstone or insert a small tube called a stent to keep the duct open. According to the GOV.UK health pages, timely intervention in biliary obstructions is essential for reducing the risk of long-term liver scarring or permanent bile duct damage. Once the duct is cleared, the bilirubin levels in the blood begin to fall, and the physical signs of jaundice gradually disappear as the liver’s drainage system is restored.
Conclusion
A blocked bile duct leads to jaundice by preventing the excretion of bilirubin, causing it to accumulate in the blood and settle in the skin and eyes. This obstructive process is often signaled by dark urine and pale stools, reflecting the redirected pathway of water-soluble bilirubin. In the UK, prompt diagnosis via imaging and resolution through procedures like ERCP are the standards of care to prevent infection and protect liver function. Understanding these mechanisms helps patients identify the significant shifts in health associated with biliary obstructions. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why is my skin itchy when my bile duct is blocked?
When bile cannot drain, bile salts build up in your blood and deposit in your skin, which can irritate nerve endings and cause persistent itching.
Can a blocked duct fix itself?
In some cases, a small gallstone might pass into the intestine on its own, but most blockages require a medical procedure to clear them safely.
Is a blocked bile duct the same as hepatitis?
No; hepatitis is inflammation of the liver cells, whereas a blocked duct is a physical obstruction in the tubes outside or within the liver.
What is a biliary stent?
A stent is a tiny plastic or metal tube placed inside the bile duct to hold it open and allow bile to flow past an obstruction.
Why do I need an MRI if I already had an ultrasound?
An ultrasound is good at seeing dilated ducts, but an MRI (MRCP) provides much more detail about the exact location and cause of the blockage.
Can I live without my gallbladder if it’s causing blockages?
Yes, once the bile duct is cleared, UK surgeons often recommend removing the gallbladder to stop more stones from causing future blockages.
What happens if a blockage is ignored?
An untreated blockage can lead to severe infection, liver damage, or a life-threatening inflammation of the pancreas.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding biliary obstructions and jaundice, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
