

The diagnosis of jaundice in adults involves a systematic clinical assessment to determine the level of bilirubin in the blood and to identify the underlying cause affecting the liver, gallbladder, or haematological system. Jaundice is a visible medical sign, rather than a disease itself, characterised by the yellowing of the skin and the whites of the eyes. When a patient presents with these symptoms in the United Kingdom, healthcare professionals follow established protocols to distinguish between different types of jaundice, such as pre-hepatic, intra-hepatic, or post-hepatic. The diagnostic pathway typically begins with a detailed medical history and a physical examination, followed by biochemical blood tests and diagnostic imaging. Because the liver performs hundreds of essential functions, identifying the specific reason for its failure to process bilirubin is necessary for effective management. UK clinical standards ensure that the investigation is comprehensive, looking for signs of infection, inflammation, or physical obstruction in the biliary tree. By using a combination of visual markers and internal diagnostic tools, clinicians can create an accurate profile of a patient’s liver and biliary health.
What We’ll Discuss in This Article
- The initial physical examination and visual assessment of jaundice.
- The role of Liver Function Tests (LFTs) in measuring bilirubin levels.
- Distinguishing between conjugated and unconjugated bilirubin through blood work.
- The use of diagnostic imaging like ultrasound and CT scans to find obstructions.
- Specialist procedures such as MRCP and ERCP for detailed duct analysis.
- How medical history and lifestyle factors inform the diagnostic process.
Physical Examination and Medical History
The diagnostic process for jaundice begins with a thorough physical examination and a review of the patient’s medical history to identify visible signs and potential risk factors. During the examination, a doctor will look for the yellowing of the skin and the sclera of the eyes, which occurs when bilirubin deposits in tissues. The NHS states that jaundice is caused by the build-up of bilirubin in the blood, and a GP will usually check for this by examining the eyes and skin in natural light.
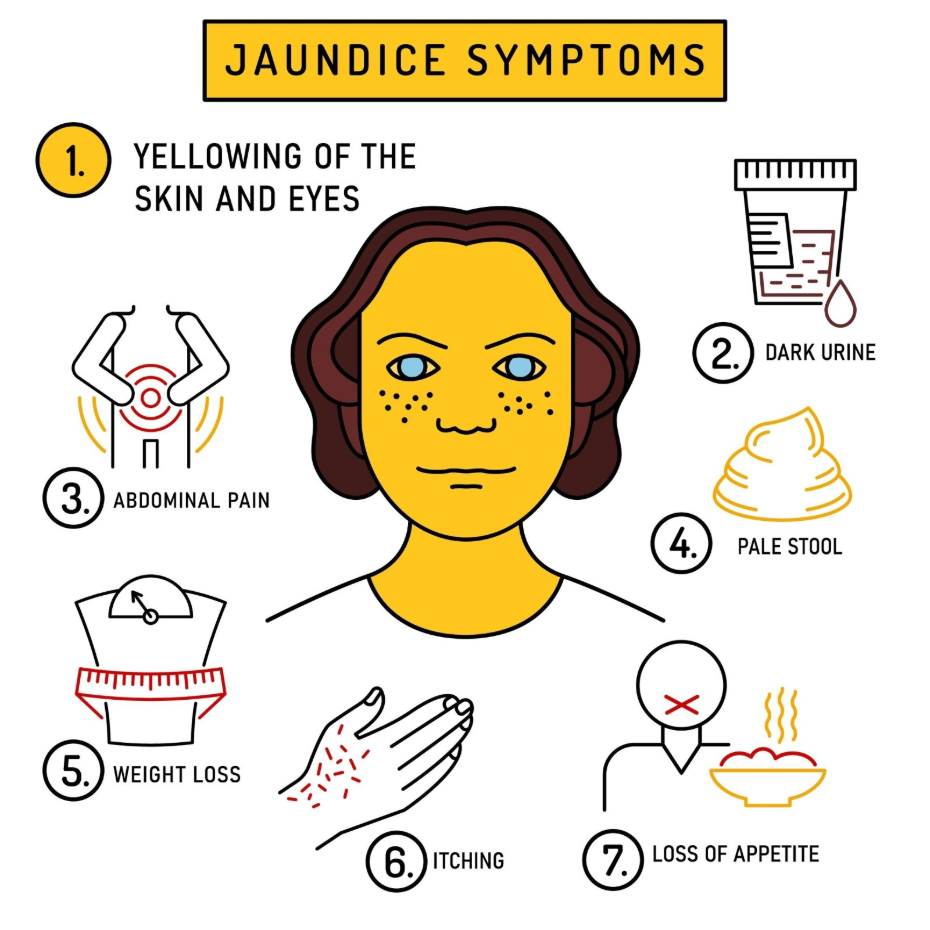
Clinicians also check for secondary physical signs that suggest liver or gallbladder distress. These may include abdominal swelling (ascites), spider naevi (small, spider-like blood vessels on the chest), or tenderness in the upper right quadrant of the abdomen. The medical history focuses on recent medications, alcohol consumption, travel history, and exposure to viral infections. Understanding the onset of symptoms—whether they appeared suddenly or gradually—helps the clinician determine if the cause is likely an acute obstruction, such as a gallstone, or a chronic condition like liver scarring.
Biochemical Blood Investigations
Blood tests, specifically Liver Function Tests (LFTs), are the primary method for confirming jaundice and categorising its origin by measuring the concentration of bilirubin and various enzymes. These tests provide a biochemical snapshot of how well the liver is processing waste and whether its cells are currently inflamed or damaged.
A standard liver profile includes several markers:
- Bilirubin: Total levels are measured to confirm the degree of jaundice.
- ALT and AST: High levels of these enzymes typically indicate direct damage to liver cells (hepatocellular injury).
- ALP and GGT: Elevations in these enzymes often suggest a problem with the bile ducts or an obstruction (cholestasis).
- Albumin and Clotting Factors: These markers show how well the liver is actually functioning as a factory for proteins.
NICE clinical guidelines for the management of liver disease emphasise that bilirubin should be “split” into conjugated and unconjugated forms during testing to help identify the source of the issue. High levels of unconjugated bilirubin often point toward blood disorders where red blood cells are breaking down too fast, whereas high conjugated bilirubin suggests the liver has processed the pigment but cannot excrete it due to damage or blockage.
Diagnostic Imaging of the Liver and Bile Ducts
If blood tests suggest a blockage or structural issue, diagnostic imaging is used to visualise the internal anatomy of the liver, gallbladder, and biliary tree. An ultrasound scan is usually the first-line imaging tool used in the UK because it is non-invasive and highly effective at detecting gallstones or widened (dilated) bile ducts.
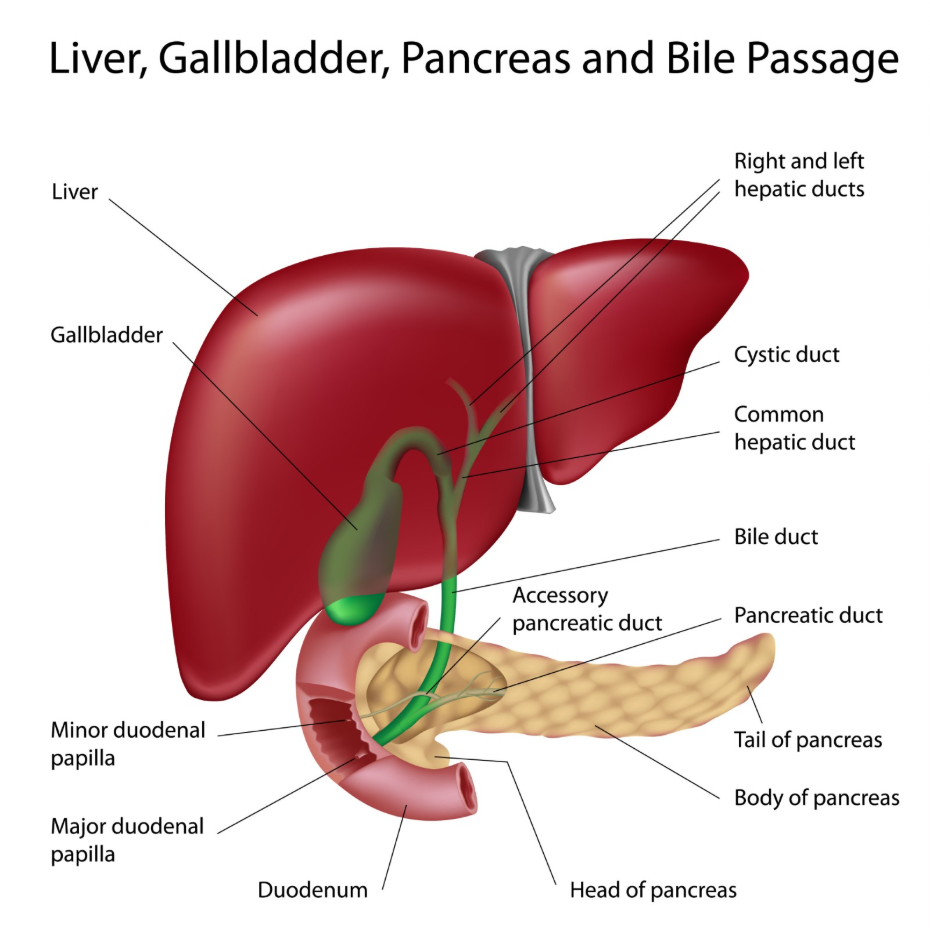
In cases where more detail is required, a CT scan or an MRI may be performed. A specific type of MRI, known as a Magnetic Resonance Cholangio-Pancreatography (MRCP), is used to create detailed images of the bile and pancreatic ducts without the need for surgery. These scans help clinicians identify tumours, cysts, or inflammation that might be compressing the drainage system.
| Imaging Tool | Primary Use | Advantage |
| Ultrasound | Checking for gallstones and duct dilation. | Quick, non-invasive, and no radiation. |
| CT Scan | Visualising liver masses or tumours. | Provides detailed cross-sectional views. |
| MRCP (MRI) | Detailed mapping of the biliary tree. | Excellent for finding small stones or narrowings. |
Advanced Endoscopic Procedures
When imaging confirms a physical obstruction in the bile ducts, advanced procedures like ERCP are used to both diagnose and treat the cause of the jaundice. Endoscopic Retrograde Cholangio-Pancreatography (ERCP) involves passing a thin, flexible tube with a camera down the throat and into the small intestine where the bile duct opens.
The GOV.UK health pages indicate that ERCP is a specialised procedure that allows clinicians to take X-rays of the bile ducts and remove obstructions like gallstones during the same session. Because it carries a small risk of complications, such as inflammation of the pancreas, it is generally reserved for cases where an obstruction is highly likely and requires intervention. This procedure is a vital part of the UK diagnostic pathway for post-hepatic jaundice, ensuring that the “plumbing” system is restored and the bilirubin can be excreted normally.
Identifying Underlying Chronic Conditions
The final stage of diagnosis often involves looking for chronic underlying conditions that may have led to the jaundice, such as viral hepatitis, autoimmune disorders, or advanced scarring. If the initial tests do not reveal a clear obstruction or acute infection, doctors may order viral serology to check for Hepatitis A, B, or C. They may also look for specific antibodies that suggest the immune system is attacking the liver tissue.
In some cases, a liver biopsy may be required. This involves taking a tiny sample of liver tissue with a needle to examine it under a microscope for signs of cirrhosis or specific cellular changes. While less common now due to the accuracy of modern scans like FibroScan, a biopsy remains the gold standard for diagnosing certain complex liver conditions. By piecing together the results of blood work, imaging, and sometimes tissue samples, the multidisciplinary healthcare team can confirm the precise cause of the jaundice and initiate the appropriate management plan.
Conclusion
Doctors diagnose jaundice through a combination of physical examination, liver function blood tests, and diagnostic imaging to identify why bilirubin levels are elevated. This process allows healthcare professionals to differentiate between blood-related, liver-related, and obstructive causes. In the UK, the focus is on rapid identification of the underlying issue to prevent further organ stress and manage symptoms like itching or pain. Consistent clinical monitoring ensures that the patient’s liver health is supported throughout the diagnostic journey. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why do I need a blood test if my skin is clearly yellow?
The blood test confirms the exact bilirubin level and measures other enzymes that tell the doctor if the problem is in your liver cells or your bile ducts.
Can an ultrasound miss a gallstone?
While ultrasound is very accurate, small stones in the common bile duct can sometimes be hidden, which is why an MRI (MRCP) might be needed next.
Is the diagnostic process the same for everyone?
The basic steps are similar, but a doctor may order different tests based on your age, symptoms, and whether you have pain or fever.
How long does it take to get a diagnosis?
Blood results are often available within 24 hours, but imaging and specialist reviews can take several days depending on the urgency.
Do I have to stay in the hospital for these tests?
Many initial tests can be done as an outpatient, but if your symptoms are severe or suggest a major blockage, you may be admitted for faster investigation.
What is a “split” bilirubin test?
This is a test that shows how much of your bilirubin has been processed by the liver, which helps doctors see if the problem is “before” or “after” the liver.
Will a scan show if I have hepatitis?
A scan shows the physical structure of the liver, but blood tests are usually needed to find the specific virus or inflammation causing hepatitis.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the diagnosis of jaundice in adults, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
