

The majority of people with fatty liver disease do not progress to cirrhosis, as the condition often remains in its earliest and least harmful stage for many years or even a lifetime. Fatty liver disease, clinically known as non-alcoholic fatty liver disease, is a spectrum of conditions where the common factor is the accumulation of excess fat within liver cells. While the presence of fat indicates a metabolic imbalance, it does not automatically result in permanent organ damage or scarring. In the United Kingdom, healthcare strategies focus on identifying the minority of patients whose condition shows signs of active inflammation, as this is the primary driver of progression toward advanced liver disease. For most individuals, the liver remains functional and the condition is reversible or manageable through consistent lifestyle adjustments. Understanding the distinction between simple fat accumulation and progressive inflammation is essential for assessing long term health risks and maintaining liver function.
What We’ll Discuss in This Article
- The distinction between simple fatty liver and progressive inflammation.
- The statistical likelihood of developing advanced liver scarring.
- Biological and metabolic factors that drive disease progression.
- The role of the immune system in triggering liver cell damage.
- How the liver’s regenerative capacity can prevent permanent scarring.
- UK clinical pathways for identifying and monitoring high risk patients.
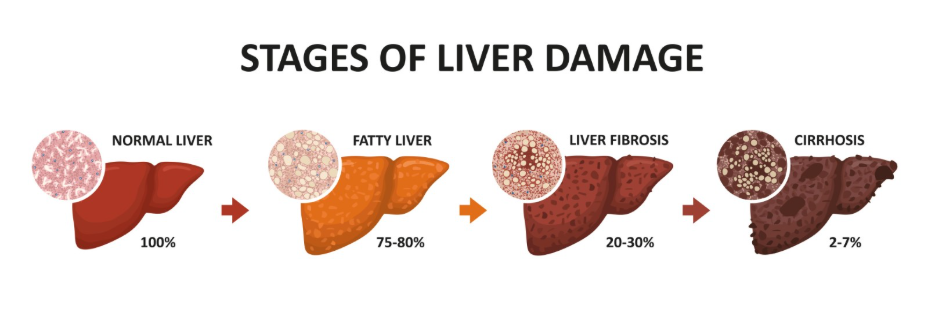
Simple Steatosis versus Progressive Inflammation
Most cases of fatty liver disease stay at the stage of simple steatosis, where fat is present in the cells but there is no significant inflammation or damage to the organ. In this state, the liver continues to perform its thousands of daily functions, and the risk of developing cirrhosis remains very low. The NHS states that non-alcoholic fatty liver disease is often divided into 4 stages, and most people will only ever develop the first stage, which is usually not serious if managed.
The condition only becomes a concern for cirrhosis when it moves into the second stage, known as non-alcoholic steatohepatitis. This stage is characterised by the liver becoming inflamed and cells being injured. It is this active inflammation, rather than the fat itself, that signals the start of the scarring process. By monitoring liver health through blood tests and scans, UK clinicians aim to differentiate between those with “quiet” fat and those with “active” inflammation to provide the appropriate level of intervention.
The Statistical Reality of Progression
Clinical data suggests that only a small proportion of the population with fatty liver disease will eventually develop the extensive scarring known as cirrhosis. While fatty liver is common in the UK, the transition to advanced disease typically takes decades and requires a combination of persistent metabolic stress and genetic susceptibility. Most individuals diagnosed with the condition will find that it remains stable or improves if the underlying metabolic drivers, such as high blood sugar or weight, are addressed.
The progression is not inevitable because the liver is an extremely resilient organ that can tolerate a certain amount of metabolic stress. Statistics show that while many people may have some degree of liver fat, only a fraction will experience the specific inflammatory triggers that lead to fibrosis (scarring). This underscores the importance of not viewing a fatty liver diagnosis as a definitive path to liver failure, but rather as an opportunity for preventative health measures.
Factors That Influence Disease Progression
Whether or not fatty liver disease progresses to cirrhosis depends on several interconnecting factors, primarily related to how the body handles insulin and energy. Metabolic conditions such as type 2 diabetes, high blood pressure, and high cholesterol act as “accelerants” that can push the liver from simple fat storage into an inflammatory state. When these conditions are poorly managed, the liver is under constant stress, which increases the likelihood of cell death and subsequent scarring.
| Condition Stage | Characteristics | Progression Risk |
| Simple Fatty Liver | Fat in cells; no inflammation | Very Low |
| Steatohepatitis (NASH) | Fat plus active cell damage | Moderate |
| Fibrosis | Initial formation of scar tissue | High if unmanaged |
| Cirrhosis | Extensive, permanent scarring | Advanced Stage |
Genetic factors also play a role in determining why some people develop cirrhosis while others with similar lifestyles do not. Some individuals carry specific gene variants that make their liver cells more sensitive to fat-induced injury. In the UK, medical assessments take these risk factors into account to create a personal risk profile for the patient, ensuring those with higher metabolic burdens receive more frequent clinical oversight.
The Liver’s Capacity for Repair and Regeneration
One of the primary reasons many cases do not reach cirrhosis is the liver’s unique ability to repair itself when the source of injury is reduced. Unlike many other organs, the liver can regenerate healthy cells and even break down early-stage scar tissue if the environment within the organ improves. This means that if an individual reduces the amount of fat being sent to the liver through weight loss or dietary changes, the progression of the disease can be halted or even reversed.
NICE clinical guidelines highlight that weight loss is the most effective way to reduce liver fat and stop the progression of inflammation in people with non-alcoholic fatty liver disease. As long as the liver has not reached the stage of advanced cirrhosis, it retains a significant capacity to heal. This biological resilience serves as a natural buffer that prevents many cases of fatty liver from ever becoming a life-threatening structural problem.
Clinical Monitoring and Early Detection in the UK
The UK healthcare system uses a tiered approach to monitoring fatty liver disease, specifically designed to catch the small number of people whose condition is progressing. This involves using non-invasive tests like the FibroScan to measure the stiffness of the liver, which is a direct indicator of whether scar tissue is forming. If the liver remains soft, it confirms that the disease is not progressing toward cirrhosis.
According to the GOV.UK health pages, proactive management of obesity and type 2 diabetes is the primary public health strategy for reducing the number of people who progress to advanced liver disease. By focusing on these systemic issues, clinicians can effectively “starve” the inflammatory process, ensuring the liver stays in the simple, non-progressive stage. Regular monitoring allows for timely intervention if a patient’s risk profile changes, providing a safety net that keeps the majority of patients away from advanced complications.
Conclusion
Not every case of fatty liver disease progresses to cirrhosis, and for the majority of people, the condition remains in a stable and non-serious stage. Progression is driven by active inflammation and metabolic stress rather than the mere presence of fat, and many individuals can reverse early-stage damage through lifestyle changes. The liver’s natural ability to regenerate and the effectiveness of modern clinical monitoring mean that advanced scarring is a preventable outcome for most patients. Maintaining good metabolic health is the most reliable way to ensure the liver remains functional and healthy over the long term.
Does having a fatty liver mean I will eventually need a transplant?
No, the vast majority of people with fatty liver disease will never reach a stage where a transplant is necessary.
Can I have fatty liver for my whole life without it getting worse?
Yes, many people live for decades with simple fatty liver that never progresses to inflammation or scarring.
Is the damage always permanent if it starts to scar?
Early-stage scarring (fibrosis) is often reversible if the underlying cause is addressed, though advanced cirrhosis is generally permanent.
Why do some people get cirrhosis while others don’t?
It depends on a combination of factors, including how well metabolic conditions like diabetes are managed, genetics, and lifestyle habits.
Will my liver blood tests always show if the disease is progressing?
Blood tests are a good indicator of inflammation, but scans like a FibroScan are more accurate for measuring the actual level of scarring.
Does alcohol affect how quickly fatty liver becomes cirrhosis?
Yes, consuming alcohol when you already have a fatty liver can significantly accelerate the inflammatory process and lead to faster scarring.
How much weight do I need to lose to help my liver?
Losing even 5% to 10% of your body weight can significantly reduce the amount of fat and inflammation in the liver.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the progression of liver disease, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in internal medicine, surgery, and emergency care. All information follows current UK public health standards to ensure accuracy and patient safety.
