

Chronic Hepatitis B is a primary risk factor for the development of hepatocellular carcinoma, the most common type of primary liver cancer. The virus increases cancer risk through a combination of persistent inflammation, the formation of scar tissue, and direct interference with the genetic material of liver cells. In the United Kingdom, healthcare strategies for managing chronic Hepatitis B focus on regular monitoring and antiviral treatment to suppress the virus, thereby reducing the likelihood of malignant changes. Understanding the biological mechanisms behind this risk is essential for patients to engage effectively with long term surveillance and preventative care provided by the NHS.
What We’ll Discuss in This Article
- The biological mechanisms by which the virus damages liver cell DNA.
- The role of chronic inflammation and cirrhosis in cancer development.
- How viral replication levels influence long term cancer risk.
- UK clinical guidelines for liver cancer surveillance in chronic patients.
- The impact of antiviral treatments on reducing cancer likelihood.
- Lifestyle factors that may further influence liver health.
Viral Integration and Genetic Damage
Chronic Hepatitis B increases liver cancer risk because the virus can integrate its own genetic material into the DNA of the host’s liver cells, causing mutations that lead to uncontrolled cell growth. When the virus inserts itself into the human genome, it can disrupt genes that normally protect the body against cancer or activate genes that promote tumour formation. The NHS notes that chronic hepatitis B can lead to serious liver damage over time, including an increased risk of developing liver cancer.
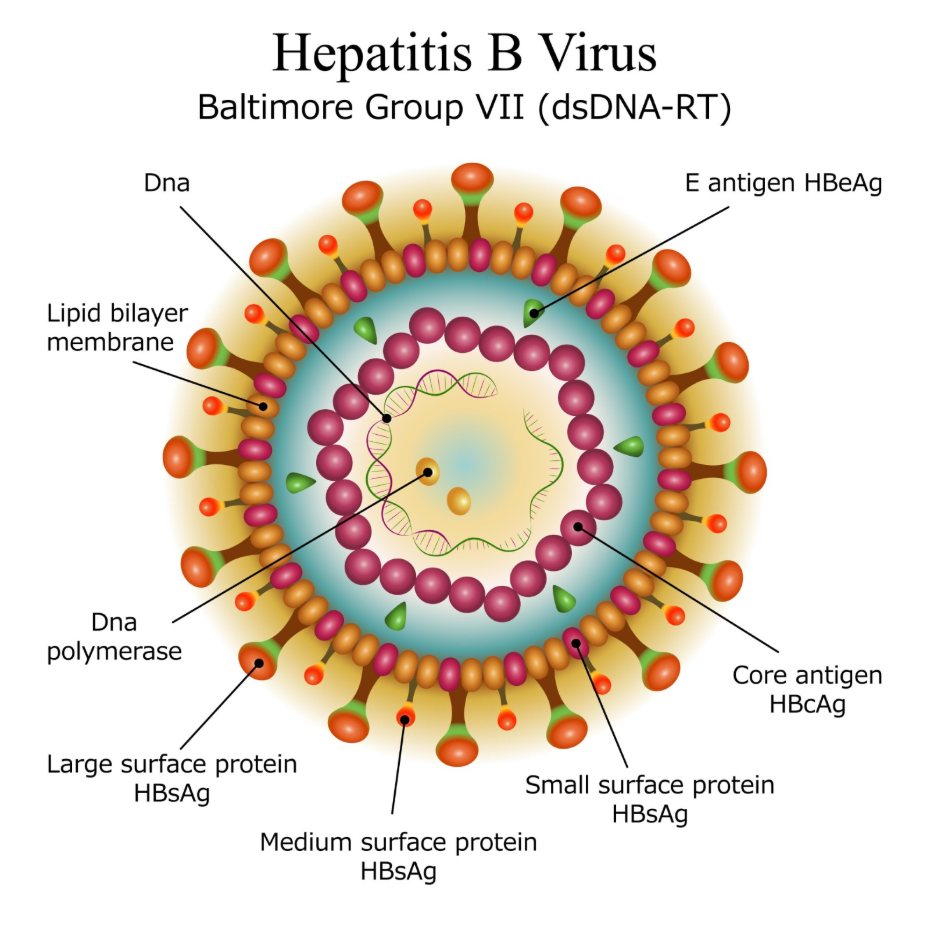
Unlike some other causes of liver cancer, Hepatitis B can sometimes trigger malignant changes even before significant scarring has occurred. The presence of the viral protein known as the X protein can interfere with cell repair mechanisms and cell death cycles. This direct genetic interference means that the virus acts as a carcinogen at a cellular level, making consistent viral suppression a priority in clinical management.
The Role of Chronic Inflammation and Cirrhosis
Persistent inflammation caused by the immune system’s attempt to clear the virus leads to a continuous cycle of cell death and regeneration that increases the chance of cancerous mutations. As the liver constantly tries to repair itself, it produces fibrous scar tissue, a process known as fibrosis. When this scarring becomes extensive, it is called cirrhosis, which significantly alters the liver’s structure and blood flow.
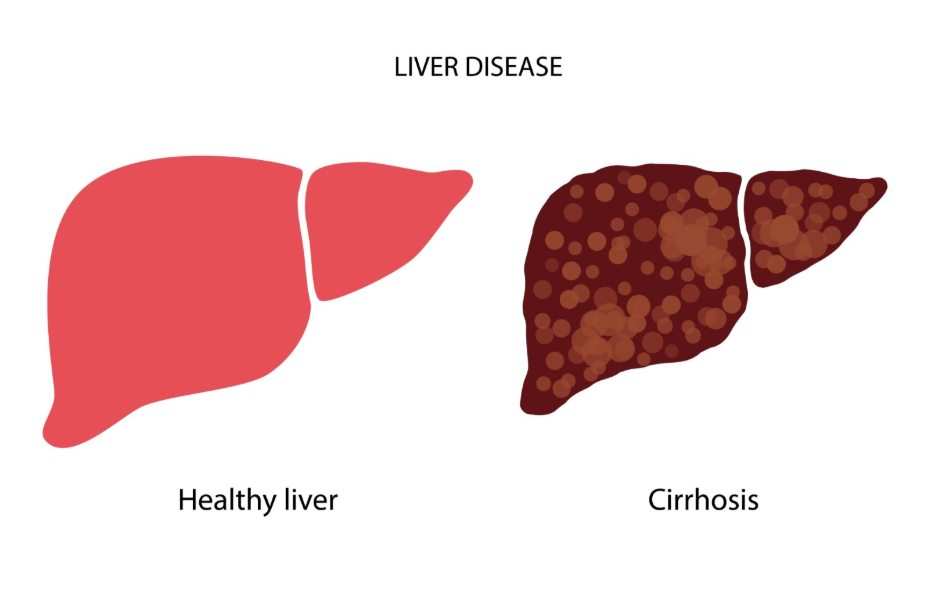
NICE guidelines state that individuals with cirrhosis caused by chronic hepatitis B are at the highest risk for hepatocellular carcinoma and require regular surveillance. The stiff, scarred environment of a cirrhotic liver promotes the survival of abnormal cells. While cancer can occur without cirrhosis in Hepatitis B patients, the presence of advanced scarring increases the statistical risk substantially, necessitating six monthly ultrasound scans for those in this high risk category.
Viral Load and Replication Levels
The risk of developing liver cancer is closely linked to the amount of virus present in the blood, often referred to as the viral load or Hepatitis B DNA level. Higher levels of viral replication are associated with increased inflammation and a higher frequency of viral integration into the host DNA. Patients with high viral loads over many years are statistically more likely to develop liver complications than those with low or undetectable levels.
| Viral Status | General Impact on Risk |
| High Viral DNA | Increased inflammation and higher cancer risk |
| Low / Undetectable DNA | Reduced inflammation and lower cancer risk |
| HBeAg Positive | Often indicates high replication and higher risk |
| HBeAg Negative | May indicate lower replication, but still requires monitoring |
Clinicians use these markers to decide when to start antiviral therapy. By using medications that stop the virus from replicating, the “insult” to the liver is reduced. Suppressing the virus to undetectable levels is the primary goal of treatment in the UK, as this has been shown to slow the progression of liver damage and decrease the probability of cells turning cancerous.
Surveillance and Early Detection in the UK
Regular surveillance is the standard of care in the UK for those at increased risk of liver cancer due to Hepatitis B. This typically involves an ultrasound scan of the liver and a blood test for a protein called alpha-fetoprotein (AFP) every six months. The objective of surveillance is to detect small tumours at an early stage when they are much easier to treat with surgery or other localised therapies.
The UK Health Security Agency provides guidance on the long term monitoring of chronic hepatitis B to ensure that complications like liver cancer are identified early. Surveillance is generally recommended for all patients with cirrhosis, as well as certain other groups based on age, family history of liver cancer, and ethnic background. Adhering to this schedule is vital because early stage liver cancer often produces no symptoms, and waiting for pain or jaundice to appear may mean the cancer is more advanced.
Impact of Antiviral Treatment on Risk Reduction
Antiviral medications are highly effective at reducing the risk of liver cancer by keeping the virus at very low or undetectable levels. While these treatments do not usually “cure” the infection by removing every trace of the virus, they effectively put the virus into a dormant state. This stops the ongoing inflammatory damage and allows the liver an opportunity to stabilise or even improve.
Research has shown that patients who remain on consistent antiviral therapy have a significantly lower incidence of liver cancer compared to those with uncontrolled viral replication. However, it is important to note that the risk is not reduced to zero, especially if significant scarring was already present before treatment began. This is why medical check ups continue even when the virus is well controlled and the patient feels healthy.
Conclusion
Chronic Hepatitis B increases liver cancer risk through direct genetic mutations and the long term effects of chronic inflammation and cirrhosis. While the virus is a significant risk factor, modern UK medical care offers effective ways to manage this risk through antiviral therapy and regular ultrasound surveillance. Early detection and viral suppression remain the most effective strategies for protecting liver health in those living with the virus. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does everyone with chronic Hepatitis B get liver cancer?
No, only a minority of people with chronic Hepatitis B will develop liver cancer; the risk is managed through monitoring and treatment.
Can liver cancer be prevented if I take my medication?
Taking antiviral medication significantly lowers the risk, but regular screening is still necessary to monitor the liver.
Why do I need a scan every six months?
Liver tumours can grow relatively quickly, so six monthly intervals are designed to catch any changes while they are still small and treatable.
Does the virus cause cancer or does the scarring?
Both play a role; the virus can cause DNA damage directly, while the scarring (cirrhosis) creates an environment that promotes tumour growth.
Can lifestyle changes help lower my risk?
Yes, avoiding alcohol and maintaining a healthy weight can reduce additional stress on the liver, complementing your medical treatment.
Is the risk the same for Hepatitis C?
Both increase cancer risk, but Hepatitis C is more likely to cause cancer only after cirrhosis has developed, whereas Hepatitis B can occasionally cause it earlier.
What is the AFP blood test?
AFP is a protein that can be produced by liver cancer cells; while not perfect, it is used alongside ultrasound to help identify potential issues.
Authority Snapshot (E-E-A-T)
This article provides medically factual health information regarding Hepatitis B and liver cancer, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in internal medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
