

Doctors determine the underlying cause of jaundice by following a structured diagnostic pathway that categorises the condition into pre-hepatic, intra-hepatic, or post-hepatic origins based on physical findings and clinical investigations. Jaundice is a visible sign of an accumulation of bilirubin in the bloodstream, but because this buildup can result from diverse issues ranging from blood disorders to biliary obstructions, a precise identification of the source is essential. In the United Kingdom, healthcare professionals utilise a combination of detailed medical history, physical examinations, biochemical blood profiles, and non-invasive imaging to narrow down the cause. The liver serves as the primary hub for processing bilirubin, so any disruption in its filtration or drainage capacity will manifest as yellowing of the skin and eyes. By systematically ruling out various triggers, clinicians can ensure that the management plan specifically addresses the core medical issue rather than just the visible symptoms. This rigorous approach is necessary to support long-term organ health and prevent complications associated with impaired liver or gallbladder function.
What We’ll Discuss in This Article
- The clinical classification of jaundice based on its biological origin.
- The role of physical examination in identifying secondary symptoms.
- How Liver Function Tests help differentiate between cell damage and blockage.
- The importance of measuring conjugated versus unconjugated bilirubin.
- When diagnostic imaging like ultrasound or CT scans is required.
- The use of specialist procedures to investigate the biliary drainage system.
Initial Clinical Classification and Assessment
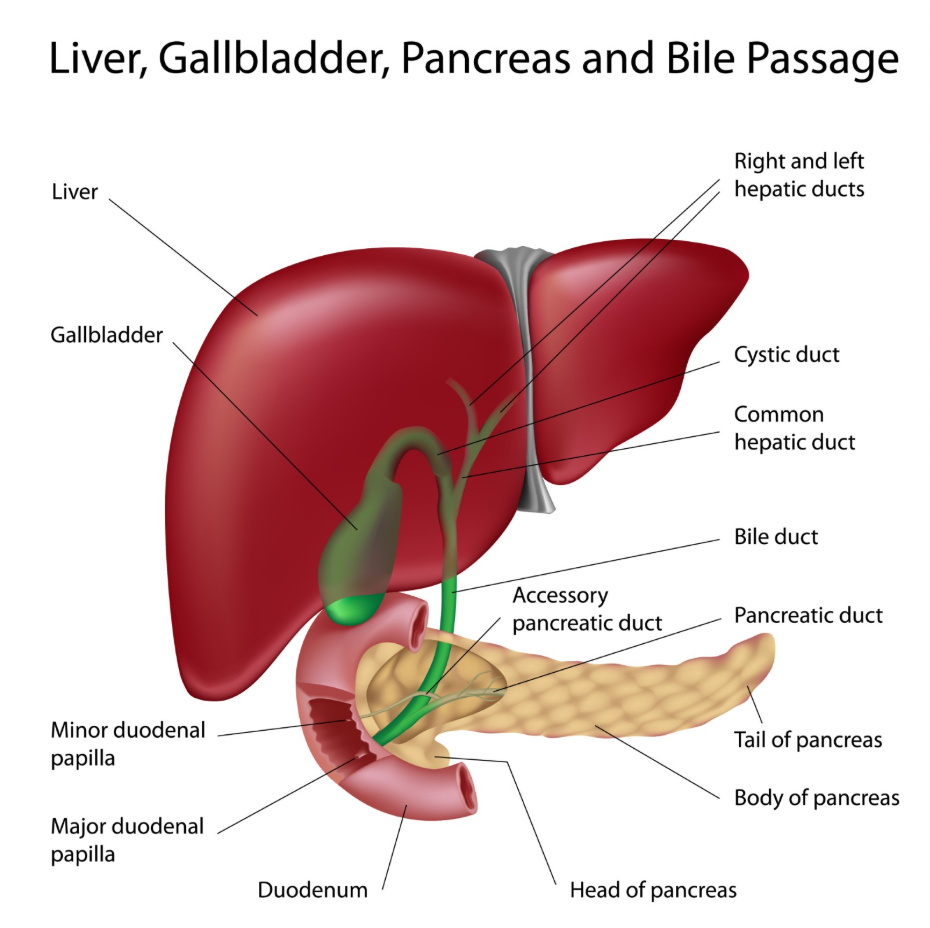
The first step doctors take to determine the cause of jaundice is to classify the condition based on where the disruption in the bilirubin cycle is occurring. Bilirubin is produced when old red blood cells are broken down, and it must pass through the liver to be excreted in bile. The NHS states that jaundice is caused by the build-up of bilirubin in the blood, which can happen if the liver is damaged or if there is a problem with the bile ducts.
By categorising the jaundice into three main types, clinicians can focus their search:
- Pre-hepatic: The problem occurs before the liver, usually due to the rapid breakdown of red blood cells.
- Intra-hepatic: The issue is within the liver itself, such as inflammation from a virus or scarring.
- Post-hepatic: The disruption is after the liver, typically a physical blockage in the bile ducts.
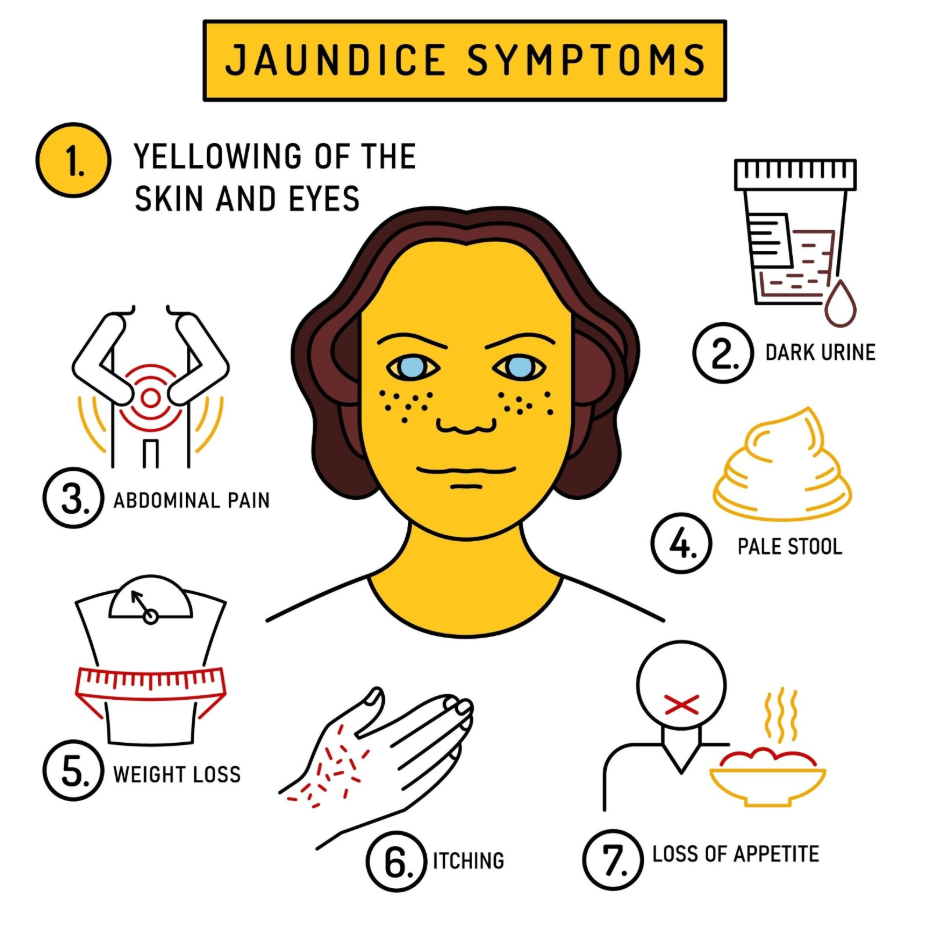
This framework allows the medical team to prioritise specific tests. For example, if a patient has no abdominal pain but has a history of anaemia, the focus may be on blood disorders. If the patient has dark urine and pale stools, the search pivots toward an obstruction in the drainage system.
Physical Examination and Symptom Review
A thorough physical examination is used to look for visible clues that suggest a specific organ is under stress, helping the doctor narrow down the diagnostic possibilities. Beyond the yellowing of the skin and the sclera of the eyes, clinicians look for signs of liver failure or biliary disease.
Doctors will typically check for:
- Abdominal Tenderness: Pain in the upper right side can suggest gallstones or liver inflammation.
- Liver or Spleen Size: An enlarged liver or spleen can indicate chronic disease or blood disorders.
- Skin Changes: The presence of spider naevi (spider-like blood vessels) or redness of the palms can be signs of liver scarring.
- Fluid Retention: Swelling in the legs or abdomen (ascites) suggests advanced liver dysfunction.
The review of symptoms also includes a history of travel, medication use, and alcohol consumption. This information is vital in the UK for distinguishing between an acute viral infection and chronic toxic damage. A sudden onset of yellowing accompanied by fever often points toward an infection, while a gradual change may suggest a long-term metabolic issue.
Interpreting Liver Function Blood Tests
Blood tests are the primary tool used to confirm jaundice and determine if the cause is related to liver cell damage or a biliary obstruction. These tests, known as Liver Function Tests, measure the levels of different enzymes and proteins in the blood. NICE clinical guidelines for jaundice in adults emphasise that interpreting the pattern of enzyme elevation is essential for distinguishing between hepatocellular injury and cholestasis.
| Enzyme / Marker | High Levels Suggest | Clinical Category |
| Bilirubin | Confirms the presence of jaundice | General Indicator |
| ALT and AST | Damage to the actual liver cells | Intra-hepatic |
| ALP and GGT | Blockage or inflammation of bile ducts | Post-hepatic |
| Albumin | Reduced ability of the liver to make proteins | Chronic Disease |
If ALT and AST are significantly higher than ALP, the cause is likely an “intra-hepatic” issue like hepatitis. If ALP and GGT are much higher than the other enzymes, it suggests a “post-hepatic” blockage such as a gallstone. This biochemical map is essential for deciding whether the patient needs a specialist in liver medicine or a specialist in the biliary system.
Distinguishing Bilirubin Types
Doctors use a “split” bilirubin test to determine whether the bilirubin in the blood is conjugated or unconjugated, which provides a definitive clue about where the processing has failed. Unconjugated bilirubin is the raw pigment that has not yet been processed by the liver. Conjugated bilirubin is the form that has been processed by the liver but cannot be excreted.
An elevation primarily in unconjugated bilirubin suggests that the liver is being overwhelmed by too much pigment (pre-hepatic) or that the liver’s internal “conjugation” machinery is failing. In contrast, an elevation in conjugated bilirubin strongly suggests that the liver has done its job, but the pigment is backing up because it cannot drain into the intestines (post-hepatic). This distinction is a cornerstone of the UK diagnostic process, as it dictates whether the next step should be a blood specialist review or an imaging scan of the ducts.
The Role of Diagnostic Imaging
Diagnostic imaging is used when blood tests suggest a physical blockage or when a structural assessment of the liver and gallbladder is required. An ultrasound scan is usually the first-line imaging tool used in the UK because it is non-invasive and highly effective at detecting gallstones and widened bile ducts.
If the ultrasound is inconclusive or if the doctor needs a more detailed view of the pancreas and surrounding tissues, a CT (Computed Tomography) scan or an MRI may be ordered. These scans can identify tumours, cysts, or inflammation that might be pressing on the drainage tubes. The GOV.UK health profiles indicate that imaging is a critical part of the investigative pathway for identifying malignancies and obstructions in the biliary system. These visual tools allow the medical team to see the “plumbing” of the liver and gallbladder, providing a physical explanation for the elevated bilirubin levels.
Specialist Investigations for Biliary Drainage
In complex cases, specialist procedures are used to provide a detailed map of the bile ducts and even allow for the removal of obstructions. A procedure called MRCP is a specific type of MRI that focuses entirely on the bile and pancreatic ducts. If an obstruction is found, an ERCP (Endoscopic Retrograde Cholangio-Pancreatography) may be performed.
During an ERCP, a flexible tube with a camera is passed down the throat into the small intestine. This allows doctors to inject dye into the ducts and take X-rays, and if a gallstone is found, it can often be removed during the same procedure. These advanced steps are typically the final part of the diagnostic journey for obstructive jaundice, ensuring that the physical cause is not only identified but also addressed to restore normal bilirubin excretion.
Conclusion
Doctors determine the cause of jaundice by using a combination of physical examination, liver function blood tests, and diagnostic imaging. By categorising the jaundice into pre-hepatic, intra-hepatic, or post-hepatic origins, healthcare professionals in the UK can systematically narrow down the source of the bilirubin buildup. Blood markers and waste product changes provide the initial evidence, while scans provide the physical confirmation of structural issues or blockages. This integrated approach ensures that the underlying condition is accurately identified and managed. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why do I need so many different blood tests for jaundice?
Different markers tell the doctor different things, such as whether your liver cells are damaged or if your bile ducts are blocked.
Can an ultrasound miss the cause of jaundice?
Yes, an ultrasound might miss small stones or certain types of liver inflammation, which is why blood tests and other scans like CT are also used.
What does it mean if my jaundice is “intra-hepatic”?
It means the problem is happening inside the liver tissue itself, such as from hepatitis, alcohol damage, or scarring.
How do doctors know if the jaundice is from a blood disorder?
They look for high levels of “unconjugated” bilirubin and check for signs of anaemia or rapid red blood cell breakdown in a full blood count.
Is a liver biopsy always needed?
No, a biopsy is only needed if other tests like scans and blood work cannot find the cause of the liver damage.
Why does the doctor ask about my travel history?
Certain types of viral hepatitis are more common in different parts of the world, so your travel history can provide a clue to an infection.
Will my jaundice go away once the cause is found?
The jaundice will begin to fade once the underlying cause is successfully treated and the bilirubin can be cleared from your blood.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the diagnosis of jaundice, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
