Depression is a clinical health condition characterised by persistent biological and psychological symptoms that significantly impair daily functioning, rather than a transient state of sadness or feeling down. In the United Kingdom, healthcare professionals recognise depression as a complex disorder involving neurochemical changes, physical symptoms, and cognitive shifts. By utilising integrated NHS support pathways, individuals can access evidence-based treatments tailored to their specific biological and functional needs for long-term recovery.
What We’ll Discuss in This Article
- The biological differences between clinical depression and transient sadness.
- How depression influences neurotransmitter regulation and brain function.
- The physical symptoms and systemic markers of a depressive disorder.
- Distinguishing between emotional fluctuations and persistent clinical episodes.
- The role of the hypothalamic-pituitary-adrenal axis in mood regulation.
- Accessing integrated NHS support for managing depression in the UK.
Biological Differences Between Sadness and Depression
Clinical depression differs from sadness because it involves prolonged physiological dysregulation that affects the body’s autonomic nervous system and metabolic processes for an extended period. While sadness is often a proportionate response to a specific event that resolves over time, depression persists regardless of circumstances and manifests through objective physical changes. The NHS states that depression is more than just feeling unhappy or fed up for a few days and is a genuine health condition.
In the United Kingdom, clinicians assess depression by looking for a cluster of symptoms that persist for at least two weeks. This professional framework provides a stable foundation for the health journey by identifying that depression has roots in the central nervous system. By utilised these integrated pathways, the healthcare system ensures that every person’s profile is supported through evidence-based understanding. This coordinated effort prioritises the safety of the individual within a validated medical environment.
Neurotransmitter Regulation and Brain Function
Clinical depression is linked to the dysregulation of chemical messengers in the brain, such as serotonin, norepinephrine, and dopamine, which coordinate mood, sleep, and energy levels. In the United Kingdom, research focuses on how these neurotransmitters interact at the synapse to maintain emotional stability. When this balance is disrupted, individuals may experience a loss of interest in previously enjoyed activities, a state known as anhedonia.
| Feature | Transient Sadness | Clinical Depression |
| Duration | Usually lasts a few days or hours. | Persists for weeks, months, or longer. |
| Physical Signs | Generally mild or situational. | Significant changes in sleep and appetite. |
| Energy Levels | Mostly maintained or fluctuates. | Persistent fatigue or leaden heaviness. |
| Functioning | Can still perform most daily tasks. | Significant impairment in work or social life. |
| Trigger | Usually linked to a specific event. | May occur without an obvious cause. |
In the UK, these biological changes are managed through integrated care plans that prioritise a person-centred approach. Identifying that low energy or “brain fog” is a biological response to neurochemical shifts helps the multidisciplinary team select the most effective management strategy. This professional oversight is essential for providing a safe and accurate understanding of the individual’s functional capability. By building a robust evidence base through clinical review, the healthcare system provides a secure environment for long-term health.
Physical Symptoms and Systemic Markers
Depression often presents with a range of physical symptoms that demonstrate the systemic nature of the condition, affecting everything from digestive health to immune function. In the United Kingdom, healthcare professionals monitor these physical markers to ensure that management strategies address the whole body rather than just the emotional state. The GOV.UK health pages provide clinical profiles indicating that the monitoring of social and cognitive challenges is a priority for ensuring integrated support.
Common physical markers identified in the UK include:
- Sleep Disruption: Difficulty falling asleep, staying asleep, or sleeping too much.
- Appetite Changes: Significant weight loss or gain unrelated to dieting.
- Psychomotor Retardation: Slowed speech, movement, or a visible lack of physical energy.
- Unexplained Pain: Persistent headaches, muscle aches, or digestive issues without a clear physical cause.
- Leaden Paralysis: A sensation of heaviness in the limbs that makes movement feel exhausting.
- Autonomic Changes: Alterations in heart rate or breathing patterns during non-active periods.
In the UK, identifying these indicators early is vital for preventing the functional decline that often accompanies chronic health challenges. The integrated support framework encourages a strengths-based approach, focusing on what the individual needs to remain healthy. By utilised these professional frameworks, the healthcare system provides a secure environment for building professional and personal confidence. These strategies aim to work with the individual’s biology to restore a sense of calm.
The Stress Response and Hormonal Regulation
The hypothalamic-pituitary-adrenal (HPA) axis plays a critical role in depression by regulating the body’s response to stress through the release of hormones like cortisol. In the United Kingdom, specialists recognise that chronic activation of this axis can lead to a state of biological exhaustion, which contributes to the persistent low mood and lack of resilience seen in clinical depression.
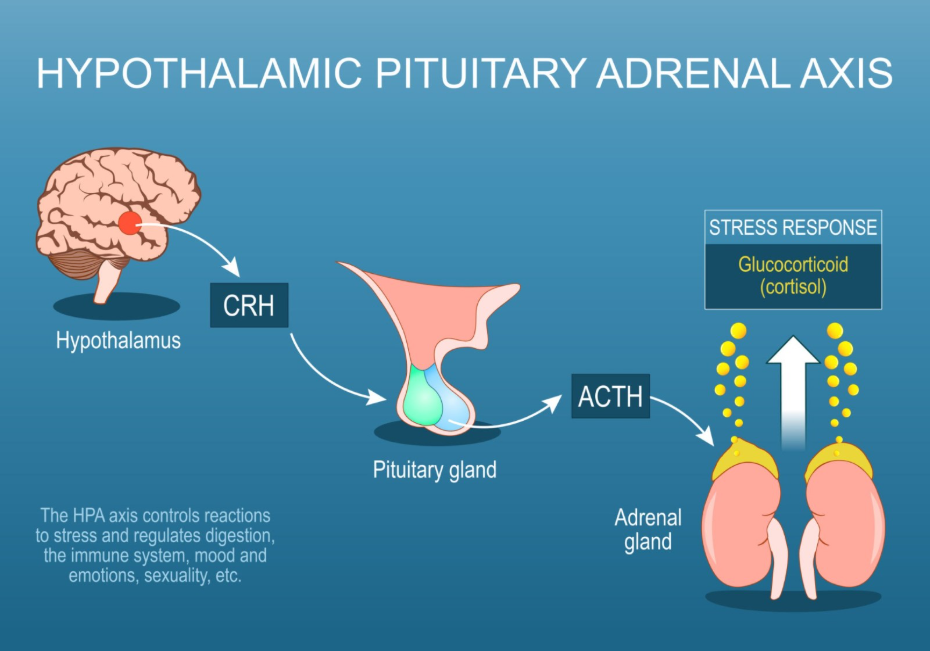
When the stress response system is overactive, it can negatively impact the hippocampus, the part of the brain involved in memory and learning. In the UK, the focus is on providing a stable foundation where the individual’s environment is reviewed alongside their metabolic health. Identifying these underlying drivers allows for more targeted help that addresses the actual biological cause of distress. By utilised these professional frameworks, the UK system provides a life-long framework of support that adapts to the person’s needs. This approach ensures that the person’s unique way of functioning is respected within their home and work environment.
Accessing Integrated NHS Support Pathways
The pathway for managing depression in the United Kingdom is a coordinated process involving primary care and specialist talking therapy services. This journey ensures that every individual receives a thorough review of their history and current environment to build a bespoke recovery plan that supports their long-term wellness. NICE clinical guidelines for common mental health problems indicate that a thorough assessment should consider the impact of depression on an individual’s social and professional life.
The UK integrated support pathway involves:
- Initial GP Consultation: Discussing physical and emotional symptoms for a clinical review.
- Talking Therapies: Accessing evidence-based support such as Cognitive Behavioural Therapy (CBT).
- Physical Screening: Performing blood tests to rule out biological causes like thyroid issues or anaemia.
- Integrated Care Planning: Co-ordinating between the GP, specialist teams, and community resources.
- Regular Monitoring: Scheduled reviews to ensure that the chosen support remains effective and safe.
- Social Prescribing: Connecting individuals with community activities to improve wellbeing.
In the UK, the focus is on providing a stable foundation for the individual to move forward with self-understanding. The NHS ensures that adults and children have a consistent point of contact for their health needs while they navigate their lives. By utilised these integrated pathways, the healthcare system provides a secure environment for building long-term mental wellbeing across the UK population. These strategies aim to work with the individual’s biology to restore a sense of calm and purpose.
Conclusion
Depression is a clinical health condition involving significant biological and physical changes that distinguish it from transient sadness or feeling down. The NHS and professional bodies in the United Kingdom provide a robust system of multidisciplinary assessments to help individuals identify their needs and access evidence-based management. By focusing on both the biological roots of symptoms and the need for supportive environments, the system promotes the highest possible level of independence. Following a coordinated management plan with the help of medical and psychological experts ensures that unique adult and paediatric needs are addressed holistically.
Can I just “snap out” of depression?
No; depression is a biological condition that requires clinical management rather than willpower to resolve.
Why do I feel physically tired when I am depressed?
Depression affects your brain chemistry and stress hormones, which can lead to persistent fatigue and a lack of physical energy.
Is it normal for my appetite to change?
Yes; significant changes in appetite and weight are recognised as physical markers of a depressive episode in the UK.
Does depression affect my memory?
Yes; chronic stress and low mood can cause “brain fog” and difficulty with concentration and short-term memory.
Can a physical illness cause depression?
Yes; some physical conditions like thyroid problems or vitamin deficiencies can cause symptoms that mimic or contribute to depression.
How long do I need to feel low before it is considered depression?
In the UK, healthcare professionals usually look for symptoms that have been persistent for at least two weeks.
Who should I talk to first if I am worried?
The first point of contact in the United Kingdom is usually your GP to discuss your health and explore support options.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the nature of depression, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in multiple clinical specialties including emergency care, general surgery, and medical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
