A brain tumour can cause speech or language difficulties by physically compressing or invading the specific regions of the brain responsible for producing and understanding communication, primarily located in the left hemisphere for most individuals. Because the brain manages complex linguistic tasks through a network of specialised centres, any structural growth can disrupt the ability to find words, form sentences, or interpret spoken and written language. While speech issues can be caused by various conditions, such as a stroke or certain types of migraine, persistent or progressive language loss requires a professional clinical evaluation to rule out a mass within the skull. The UK healthcare system utilise a structured diagnostic pathway, involving high-resolution imaging and specialist reviews, to identify if a tumour is the underlying cause of such impairments. Understanding the relationship between brain health and communication is essential for patients and their families to recognise when professional medical advice is required. By following evidence-based protocols established by the NHS and NICE, clinical teams aim to manage these symptoms while addressing the physical growth to preserve the patient’s functional independence and quality of life.
What We’ll Discuss in This Article
- The biological mechanism of tumour-induced language disruption.
- The role of Broca’s area in speech production and motor control.
- How tumours in Wernicke’s area affect language comprehension.
- Distinguishing between speech muscle weakness and cognitive language loss.
- Management strategies and the role of speech and language therapy.
- UK clinical pathways for the urgent assessment of communication deficits.
Biological Mechanisms of Language Disruption
Speech and language problems occur in patients with brain tumours when the abnormal mass interferes with the neural circuits that facilitate the complex process of human communication. These circuits require the rapid transmission of electrical signals between different lobes of the brain; when a tumour is present, it can cause “oedema,” which is a build-up of fluid that puts pressure on healthy nerve fibres. The NHS states that a brain tumour can cause symptoms by increasing the pressure inside the skull or by damaging the part of the brain where the tumour is growing.
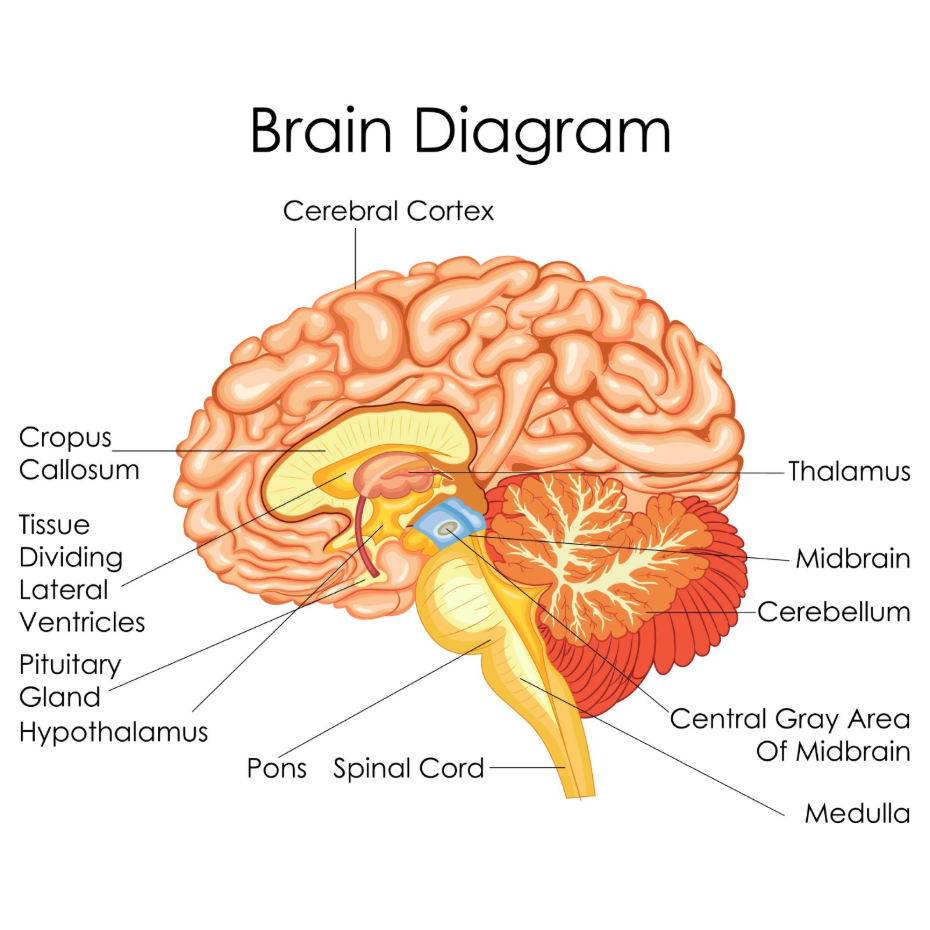
This physical disruption can slow down the brain’s ability to retrieve vocabulary or coordinate the muscles needed for articulation. Furthermore, as a tumour grows, it can interrupt the “arcuate fasciculus,” which is the white matter pathway that connects the areas responsible for understanding language with those responsible for producing it. In the United Kingdom, clinicians assess these changes to determine if they are “expressive” (difficulty speaking) or “receptive” (difficulty understanding) in nature. This distinction is vital for mapping the tumour’s exact location and determining the most appropriate management plan.
Broca’s Area and Speech Production
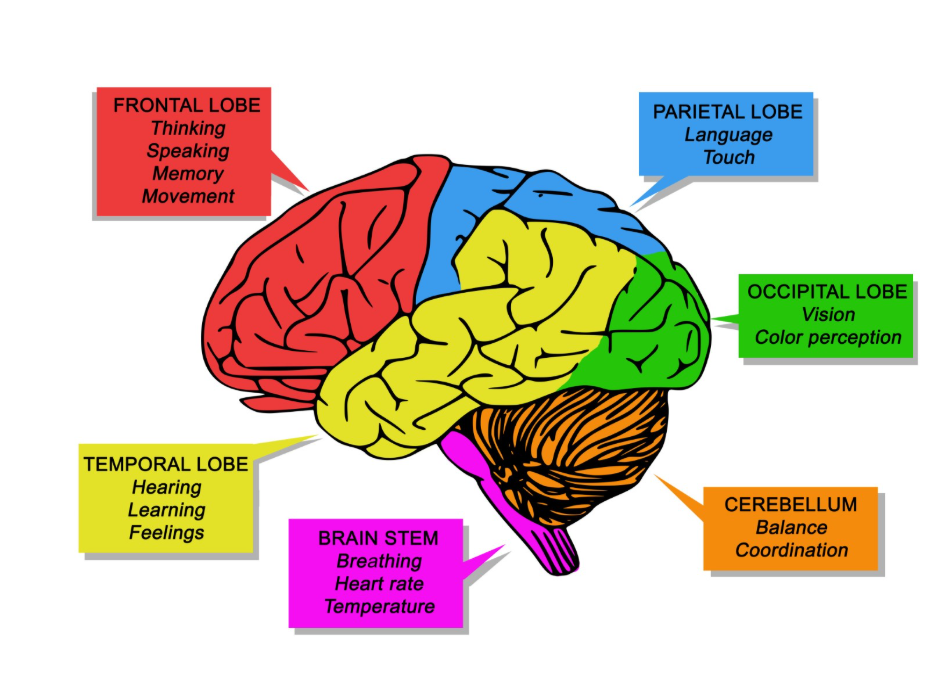
Broca’s area, located in the frontal lobe of the dominant hemisphere (usually the left), is responsible for the production of speech and the arrangement of words into grammatically correct sentences. If a tumour develops in or presses against this region, an individual may experience “Broca’s aphasia,” where they know what they want to say but struggle to physically produce the words.
Patients often speak in short, meaningful phrases that require a great deal of effort, a condition sometimes described as “telegraphic speech.” For example, a person might say “Walk dog” instead of “I am taking the dog for a walk.” In the United Kingdom, clinicians identify these deficits during a neurological examination by asking the patient to name common objects or repeat complex sentences. Because this area is also involved in the motor movements of the mouth and tongue, a tumour here can cause speech to sound slurred or hesitant. UK specialists utilise this information to prioritise imaging of the frontal regions, ensuring that any structural irritants are identified promptly.
Wernicke’s Area and Language Comprehension
Wernicke’s area, situated in the temporal lobe, is the primary region for understanding spoken and written language, making it a common site where a tumour can cause profound communication confusion. If a tumour affects this area, the individual may experience “Wernicke’s aphasia,” characterised by the ability to speak fluently but with words that make little sense or are entirely made up.
This is sometimes referred to as “word salad,” where the rhythm and pace of speech remain normal, but the content is incomprehensible. Critically, the person may also be unaware that their speech does not make sense and will struggle to understand what others are saying to them.
| Feature | Broca’s Area Disruption | Wernicke’s Area Disruption |
| Speech Output | Slow, hesitant, fragmented. | Fast, fluent, but nonsensical. |
| Understanding | Generally preserved. | Significantly impaired. |
| Self-Awareness | Often frustrated by difficulty. | Often unaware of errors. |
| Reading/Writing | May be impaired. | Typically heavily affected. |
NICE clinical guidelines for brain tumours indicate that any new-onset aphasia or persistent language difficulty should be investigated with urgent imaging to identify the cause. Understanding these anatomical differences allows the UK clinical team to provide more targeted support for the patient’s specific type of language loss.
Dysarthria versus Aphasia
In the UK clinical setting, it is important to distinguish between dysarthria, which is the physical weakness of the speech muscles, and aphasia, which is a cognitive problem with language processing. Dysarthria occurs when a tumour affects the parts of the brain that control the muscles of the lips, tongue, and throat, such as the motor cortex or the brainstem.

A patient with dysarthria has the mental language intact but sounds slurred, quiet, or breathy because the physical mechanics of speaking are compromised. Aphasia, however, is a deeper issue where the brain’s “dictionary” or “grammar centre” is damaged. The GOV.UK health pages provide clinical profiles that describe how different types of communication changes can be the presenting signs of a brain tumour. Clinicians use detailed speech assessments to make this distinction. While dysarthria might require physical exercises to strengthen muscles, aphasia management focuses on retraining the brain’s language pathways. Both conditions require a multidisciplinary approach in the UK to ensure the patient can communicate their needs effectively.
Management and Speech Therapy in the UK
Management of speech and language problems associated with a brain tumour in the United Kingdom involves a multidisciplinary approach that targets the underlying growth while providing intensive communication support. Once the tumour is addressed through surgery or other clinical methods, many patients are referred to Speech and Language Therapists (SLTs).
These specialists work with patients to rebuild their vocabulary, practice sentence structure, and develop alternative ways to communicate, such as using gesture or digital aids. In the UK, SLTs also assess swallowing function, as the same brain areas involved in speech often regulate the throat muscles. If speech issues are caused by brain swelling, medications like steroids may lead to a rapid improvement in communication as the pressure on the language centres is relieved. This comprehensive care system ensures that the patient’s ability to interact with others is prioritised alongside their physical recovery, fostering a holistic approach to neurological health.
UK Clinical Pathways for Speech Assessment
The United Kingdom uses integrated care pathways to ensure that patients reporting persistent or worsening speech problems are assessed thoroughly for structural neurological causes. This typically begins with a GP review, followed by an urgent referral under the “28-Day Faster Diagnosis Standard” if a structural brain issue is suspected.
The UK diagnostic pathway includes:
- Initial Assessment: GP review of the history of speech changes and any associated “red flag” signs.
- Neurological Exam: Checking facial symmetry, tongue movement, and language comprehension.
- Urgent Imaging: Access to CT or MRI scans to visualise the language centres of the brain.
- MDT Discussion: A Multidisciplinary Team of experts determining the best management plan for the tumour and symptoms.
This structured system ensures that serious conditions are identified early, providing a clear route for those whose communication loss is related to a brain growth. By following these national protocols, the NHS provides a safety net that catches complex neurological issues while offering reassurance and support to the patient throughout their diagnostic and management journey.
Conclusion
A brain tumour can cause significant speech or language difficulties by disrupting the specialised lobes responsible for production and comprehension, particularly the frontal and temporal lobes. These symptoms may manifest as slurred speech, difficulty finding words, or a total loss of the ability to understand language and require professional clinical evaluation. In the UK, the NHS provides a clear pathway for investigating these changes to identify if a structural growth is the underlying cause. While speech issues can be challenging, they are often managed effectively through a combination of medical treatment and specialist therapy. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does a stutter mean I have a brain tumour?
No; stammers or stutters are very rarely caused by tumours and are usually long-standing conditions or related to other health factors.
Can a brain tumour make me lose my ability to read?
Yes; tumours in the parietal or occipital lobes can interfere with the brain’s ability to interpret written symbols, a condition known as alexia.
Will my speech go back to normal after surgery?
Many patients experience a significant improvement in speech once the pressure is relieved, though some may need long-term therapy to recover full fluency.
How can I tell if my word-finding difficulty is serious?
In the UK, you should see a GP if the difficulty is persistent, getting worse, or accompanied by other issues like headaches or weakness.
Do tumours in children cause the same speech issues?
Children may show signs like a delay in reaching language milestones, a change in the clarity of their speech, or struggling with schoolwork.
Can medication cause speech problems in tumour patients?
Yes; some treatments, such as certain anti-seizure medications, can occasionally cause a feeling of “fogginess” or slightly slower speech.
Is a sudden loss of speech a “red flag” symptom in the UK?
Yes; any sudden inability to speak or understand language is a medical priority and should be assessed urgently.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding brain tumours and speech difficulties, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in emergency care, surgery, and clinical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
