Surgery is not a standard first-line treatment for the inflammation associated with pancreatitis, but it becomes a necessary intervention when specific complications or underlying causes are identified. In the United Kingdom, healthcare professionals prioritise medical management, such as fluid therapy and pain relief, to stabilise the patient first. Surgical procedures are strategically utilised to address the root cause of the inflammation, such as gallstones, or to manage severe complications where pancreatic tissue has become damaged or infected.
What We’ll Discuss in This Article
- The role of gallbladder surgery in preventing recurrent attacks.
- When surgical intervention is required for infected pancreatic necrosis.
- Procedures for managing blockages in the bile and pancreatic ducts.
- The use of surgery to drain pancreatic pseudocysts.
- Minimal access and “step-up” surgical techniques used in the NHS.
- Long-term surgical considerations for chronic pancreatic pain.
Gallbladder Removal to Prevent Recurrence
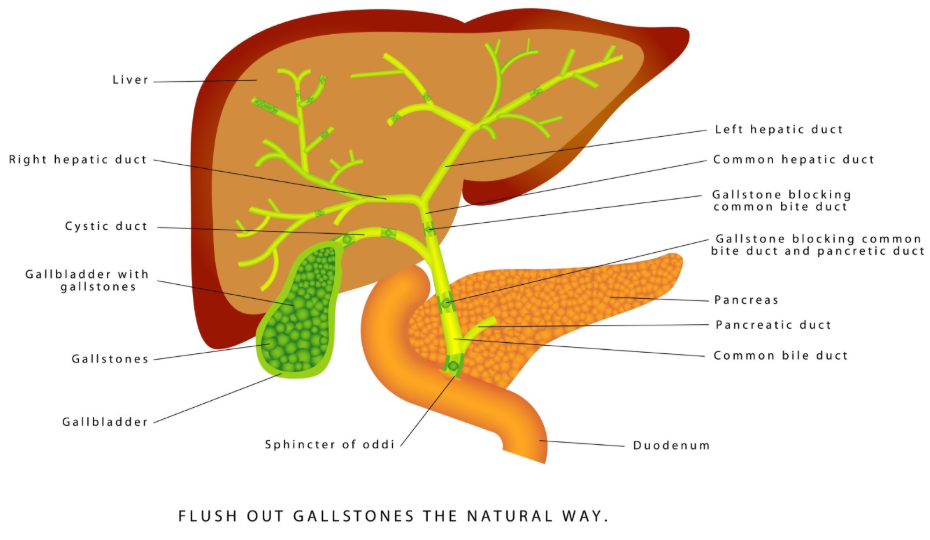
Surgery is most commonly required for pancreatitis when gallstones are identified as the primary trigger for the inflammation. If a gallstone blocks the pancreatic duct, it can cause sudden and severe inflammation. To prevent a repeat episode, which is a significant risk, the NHS often recommends the surgical removal of the gallbladder, a procedure known as a cholecystectomy.
For most patients with mild gallstone pancreatitis, this surgery is ideally performed during the same hospital admission or within two weeks of discharge. The procedure is typically done using “keyhole” or laparoscopic surgery, which involves small incisions and results in a faster recovery time compared to open surgery. By removing the source of the stones, the risk of future pancreatic inflammation is substantially reduced.
Surgery for Infected Pancreatic Necrosis
In severe cases of acute pancreatitis, parts of the pancreatic tissue may lose their blood supply and die, a condition called necrosis. Surgery is required if this dead tissue becomes infected, as antibiotics alone are often insufficient to clear the infection. This condition is serious and requires a specialised surgical approach to remove the infected material while preserving as much healthy tissue as possible.
UK clinical practice follows a “step-up” approach for managing infected necrosis. This means that doctors first attempt to drain the infection using a needle or a small tube inserted through the skin or via an endoscope. If these minimally invasive methods do not resolve the infection, a surgical procedure called a necrosectomy may be performed. Modern techniques allow many of these surgeries to be done using minimally invasive video-assisted methods, which are less stressful for the body than traditional open surgery.
Managing Duct Blockages and ERCP
While not always classified as traditional surgery, certain procedural interventions are necessary to clear blockages in the pancreatic or biliary ducts. Endoscopic Retrograde Cholangiopancreatography (ERCP) is a procedure performed by a specialist, often a gastroenterologist or surgeon, using a long, flexible camera passed through the mouth. It is used to remove gallstones that have become stuck in the common bile duct.
The use of ERCP is specifically indicated for patients who have symptoms of a blocked bile duct, such as jaundice or an infection of the bile ducts. During the procedure, the specialist may also place a small plastic or metal tube called a stent to keep the duct open. This intervention is crucial for restoring the flow of digestive juices and preventing the worsening of pancreatic inflammation.
Drainage of Pancreatic Pseudocysts
Surgery may be needed to treat pancreatic pseudocysts, which are collections of fluid and tissue debris that can form after an episode of acute pancreatitis. Many pseudocysts resolve on their own with time and monitoring, but if they become very large, painful, or infected, they must be drained. A pseudocyst can also cause problems if it presses against the stomach or other nearby organs.
Surgical drainage can be performed endoscopically, where a connection is created between the cyst and the stomach or small intestine to allow the fluid to drain internally. If endoscopic drainage is not possible or if the cyst is in a difficult location, a surgeon may perform a laparoscopic or open procedure to drain the collection. The goal is to relieve the pressure and prevent the cyst from rupturing or causing further complications.
Chronic Pancreatitis and Intractable Pain
In some cases of chronic pancreatitis, surgery is considered a last resort for managing severe and persistent pain that has not responded to medical treatments. This type of surgery often focuses on improving the drainage of the pancreatic duct or removing the most damaged parts of the organ. These procedures are complex and are usually performed in specialist hepatobiliary centres.
Examples of these surgeries include the Puestow procedure, which opens the pancreatic duct to improve flow, or a partial pancreatectomy to remove a specific scarred section of the pancreas. Because these surgeries carry risks and can affect the organ’s ability to produce insulin and enzymes, NICE guidelines recommend that surgery for chronic pancreatitis should only be considered after a thorough multidisciplinary team review.
Comparison of Surgical Interventions
The following table compares the different surgical approaches based on the clinical need.
| Procedure Type | Primary Indication | Typical Approach |
| Cholecystectomy | Gallstone-induced pancreatitis | Laparoscopic (keyhole) |
| Necrosectomy | Infected dead pancreatic tissue | Minimally invasive or “step-up” |
| ERCP | Blockage in the bile or pancreatic duct | Endoscopic (via the mouth) |
| Pseudocyst Drainage | Large, painful, or infected fluid collection | Endoscopic or laparoscopic |
| Pancreatic Resection | Severe chronic damage with intractable pain | Open or laparoscopic surgery |
Conclusion
Surgery for pancreatitis is a targeted intervention used to address specific complications or the underlying causes of inflammation. While most patients recover with medical support, procedures like gallbladder removal and the drainage of infected tissue are essential for preventing recurrence and managing severe illness. All surgical decisions are made within a multidisciplinary framework to ensure the highest safety standards for the patient. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is it safe to have surgery while my pancreas is still inflamed?
Surgeons usually prefer to wait until the initial acute inflammation has started to settle before performing surgery like gallbladder removal. However, if there is a severe infection or a life-threatening blockage, emergency surgery may be necessary.
How long is the recovery after pancreatic surgery?
Recovery time depends on the complexity of the procedure. A keyhole gallbladder removal may only require a 1 to 2 day stay, whereas a necrosectomy or major pancreatic surgery can involve several weeks of hospital recovery.
Will I need to take enzymes after part of my pancreas is removed?
If a significant portion of the pancreas is removed or if the remaining tissue is scarred, you may need to take pancreatic enzyme replacement therapy (PERT) to help you digest food.
Can a pseudocyst be treated without surgery?
Many small pseudocysts do not cause symptoms and are monitored with regular scans to see if they shrink on their own. Intervention is only needed if they grow large or cause complications.
What are the risks of pancreatic surgery?
Like all major operations, there are risks of bleeding, infection, and reactions to anaesthesia. Specifically for the pancreas, there is a risk of developing a “fistula,” where pancreatic juices leak from the surgical site.
Will removing my gallbladder cure my pancreatitis?
If gallstones were the cause of your pancreatitis, removing the gallbladder is very effective at preventing future attacks, but it does not fix any damage that has already occurred to the pancreas itself.
Authority Snapshot (E-E-A-T)
This article provides educational information about the surgical requirements for pancreatitis in the United Kingdom. All content is strictly aligned with the clinical standards of the National Health Service (NHS) and the National Institute for Health and Care Excellence (NICE). The material has been reviewed by the Medical Content Team and Dr. Stefan Petrov to ensure clinical accuracy and safety for the general public.
