Chronic diarrhoea is a persistent change in bowel habits that requires a structured diagnostic approach to identify the underlying cause and ensure appropriate management. In the UK, medical professionals follow specific clinical pathways to differentiate between functional issues, such as Irritable Bowel Syndrome, and organic conditions like Inflammatory Bowel Disease or coeliac disease. The diagnostic process typically involves a combination of non-invasive screenings, laboratory analysis of blood and stool samples, and, in some cases, more detailed internal examinations or imaging.
What We’ll Discuss in This Article
- The clinical definition of chronic diarrhoea and the initial assessment
- Essential blood tests for identifying inflammation and malabsorption
- The role of stool tests in detecting infection and inflammation
- Specific antibody testing for coeliac disease
- Advanced investigations including endoscopy and colonoscopy
- Imaging and specialised scans for malabsorption issues
Initial Clinical Assessment and History Taking
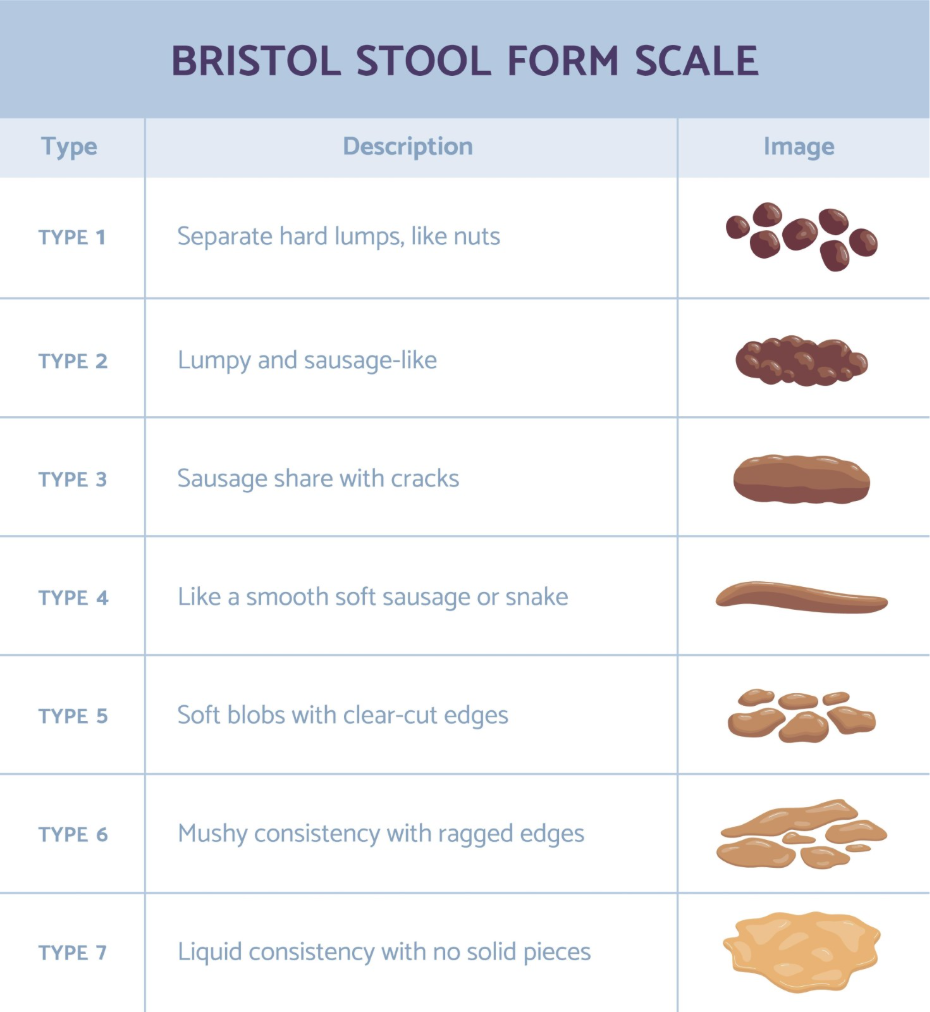
The first step in investigating chronic diarrhoea is a thorough clinical assessment where a healthcare professional reviews the duration, frequency, and nature of the bowel movements. Chronic diarrhoea is defined as the passage of loose or watery stools for a period exceeding four weeks. During this assessment, the clinician will ask about “red flag” symptoms, such as unintended weight loss, blood in the stool, or symptoms that occur during the night, as these guide the urgency of further testing.
Personal and family medical history is also critical, particularly concerning autoimmune conditions or gastrointestinal cancers. A physical examination may be performed to check for abdominal tenderness, masses, or signs of anaemia and malnutrition. This initial phase helps determine whether the symptoms are likely functional, meaning related to the way the gut works, or organic, meaning there is physical damage or inflammation present.
Common Blood Tests for Gastrointestinal Health
Blood tests are a fundamental part of the diagnostic pathway used to screen for systemic signs of disease, inflammation, and nutrient deficiencies. A Full Blood Count is often the first test requested to check for anaemia, which can be a sign of internal bleeding or malabsorption. Additionally, clinicians check markers of inflammation such as C-reactive protein (CRP) or Erythrocyte Sedimentation Rate (ESR), which are often elevated in conditions like Inflammatory Bowel Disease.
Tests for kidney and liver function, as well as electrolyte levels, help determine the systemic impact of persistent diarrhoea on the body’s hydration and chemical balance. Blood tests are used to check for signs of infection, inflammation, or anaemia and to rule out other conditions that might be causing bowel changes. If malabsorption is suspected, the clinician may also request tests for vitamin B12, folate, and ferritin levels.
Stool Analysis and the Faecal Calprotectin Test
Stool samples are essential for ruling out persistent infections and identifying whether inflammation is originating directly in the bowel. A stool culture and sensitivity test can identify parasitic or bacterial infections that have not cleared naturally. This is particularly relevant for individuals who have recently travelled abroad or who have a history of antibiotic use.
One of the most significant advancements in diagnosing bowel issues is the faecal calprotectin test. Calprotectin is a protein released by white blood cells when there is inflammation in the gastrointestinal tract. The National Institute for Health and Care Excellence recommends faecal calprotectin testing to help doctors distinguish between non-inflammatory bowel disorders like IBS and inflammatory bowel diseases like Crohn’s or colitis. This test is highly effective at reducing the need for invasive procedures in patients where inflammation is unlikely.
Screening for Coeliac Disease
Coeliac disease is a common cause of chronic diarrhoea that is identified through specific antibody testing and, in some cases, a small bowel biopsy. The primary screening tool is a blood test for Tissue Transglutaminase (tTG) antibodies. It is essential that patients continue to consume a gluten-containing diet leading up to this test, as removing gluten can lead to a false-negative result by reducing the level of antibodies in the bloodstream.
If the antibody test is positive, or if there is a high clinical suspicion despite a negative result, a referral to a gastroenterologist for a biopsy may be necessary. During this procedure, a small sample of the lining of the small intestine is taken to check for the characteristic damage to the villi. Coeliac disease is a condition where your immune system attacks your own tissues when you eat gluten, and it requires specific diagnostic steps to confirm.
Endoscopic Procedures and Colonoscopy
When non-invasive tests suggest inflammation or when red flag symptoms are present, endoscopic procedures are used to directly visualise the digestive tract. A colonoscopy involves using a thin, flexible tube with a camera to examine the entire length of the large intestine (colon) and the end of the small intestine (terminal ileum). This allow the clinician to identify ulcers, polyps, or areas of inflammation that are characteristic of Inflammatory Bowel Disease.
During these procedures, biopsies are typically taken even if the lining looks normal. This is because some conditions, such as microscopic colitis, can only be diagnosed by looking at the tissue under a microscope. A gastroscopy (upper GI endoscopy) may also be performed if the clinician needs to investigate the stomach or the beginning of the small intestine. These tests provide the most definitive evidence for organic bowel disease.
Specialised Scans for Malabsorption
In cases where standard tests are inconclusive, specialised imaging or scans may be used to investigate less common causes of chronic diarrhoea, such as bile acid malabsorption. A SeHCAT scan is the gold standard for diagnosing bile acid diarrhoea. It involves taking a small capsule containing a synthetic bile acid and then undergoing scans over the course of a week to measure how well the body retains that acid.
Other imaging modalities, such as a CT scan or MRI of the abdomen, may be used to look for structural abnormalities, issues with the pancreas, or complications of inflammatory conditions. A hydrogen breath test is another non-invasive option sometimes used to investigate lactose intolerance or Small Intestinal Bacterial Overgrowth (SIBO) by measuring the gases produced when certain sugars are fermented in the gut. These tests are usually reserved for the secondary care setting after initial primary care screenings have been completed.
Monitoring and Follow-Up Testing
Once a cause for chronic diarrhoea has been identified or ruled out, follow-up testing may be required to monitor the effectiveness of management strategies. For example, individuals with IBD may have repeat faecal calprotectin tests to check if inflammation is decreasing. For those with coeliac disease, follow-up blood tests ensure that the antibody levels are dropping, indicating successful adherence to a gluten-free diet.
If a functional disorder like IBS is suspected and all other tests are normal, the focus of future interactions will shift toward symptom management rather than further diagnostic testing. Clinicians use these test results to provide patients with clear information about their digestive health and to tailor management plans that align with national clinical standards.
Conclusion
Diagnosing the cause of chronic diarrhoea involves a systematic progression from simple blood and stool tests to more detailed investigations like colonoscopy or specialised malabsorption scans. These tests are essential for distinguishing between functional conditions and organic diseases that require specific medical treatments. Most patients will start with non-invasive screenings in primary care before any specialist referral is considered. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
How long do I need to have diarrhoea before tests are started?
In the UK, diarrhoea is considered chronic and usually requires investigation if it persists for more than four weeks without a clear cause.
Can I be tested for IBS?
IBS is generally a diagnosis of exclusion, meaning doctors use tests to rule out other conditions like coeliac disease or IBD before confirming IBS based on your symptoms.
Is a colonoscopy always necessary for chronic diarrhoea?
No, many people can be diagnosed through blood and stool tests alone; a colonoscopy is usually reserved for cases where inflammation is suspected or red flag symptoms are present.
Why do I need to keep eating gluten before a coeliac test?
The test looks for antibodies your body makes when you eat gluten; if you stop eating it, the antibodies may disappear, leading to an inaccurate result.
What does a high faecal calprotectin level mean?
A high level indicates that there is active inflammation in the bowel, which usually requires further investigation to determine if the cause is an infection or a condition like IBD.
Are there tests for food intolerances on the NHS?
The NHS primarily tests for coeliac disease and lactose intolerance; most other “food intolerance” tests sold commercially are not currently validated for clinical use.
What is a SeHCAT scan?
It is a specialised nuclear medicine scan used to determine if your diarrhoea is caused by your body’s inability to reabsorb bile acids properly.
Authority Snapshot (E-E-A-T)
This medical education content is designed to provide clear, evidence-based information to the UK public regarding the diagnostic pathways for chronic bowel changes. The material is produced by a dedicated medical content team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience across internal medicine and acute care. All information provided is strictly aligned with the clinical guidelines and diagnostic standards set by the NHS and NICE.
