Anxiety can lead to depressive episodes because the chronic physiological and psychological strain of a persistent stress response can eventually deplete the brain’s cognitive and emotional resources. In the United Kingdom, healthcare professionals recognise that long-term anxiety often acts as a significant precursor to depression, a relationship frequently observed in clinical practice as co-morbidity. When the body remains in a constant state of hyper-arousal or “fight or flight,” the resulting exhaustion can transition into the low mood, lethargy, and hopelessness characteristic of a depressive episode. By utilising integrated NHS pathways, individuals can access multidisciplinary support that addresses the progression from worry to low mood through evidence-based therapies and lifestyle adjustments. Understanding this link allows for a more factual, non-alarmist approach to mental health that prioritises early intervention and functional stability. This professional framework ensures that management strategies are safely aligned with national clinical standards within the UK health system.
What We’ll Discuss in This Article
- The biological transition from chronic stress to emotional exhaustion.
- Identifying the early indicators that anxiety is evolving into low mood.
- The role of neurotransmitter depletion in co-occurring conditions.
- How avoidance behaviours in anxiety contribute to social isolation and depression.
- Integrated NHS management strategies for complex mental health profiles.
- Accessing multidisciplinary support through primary and secondary care.
The Biological Path from Anxiety to Depression
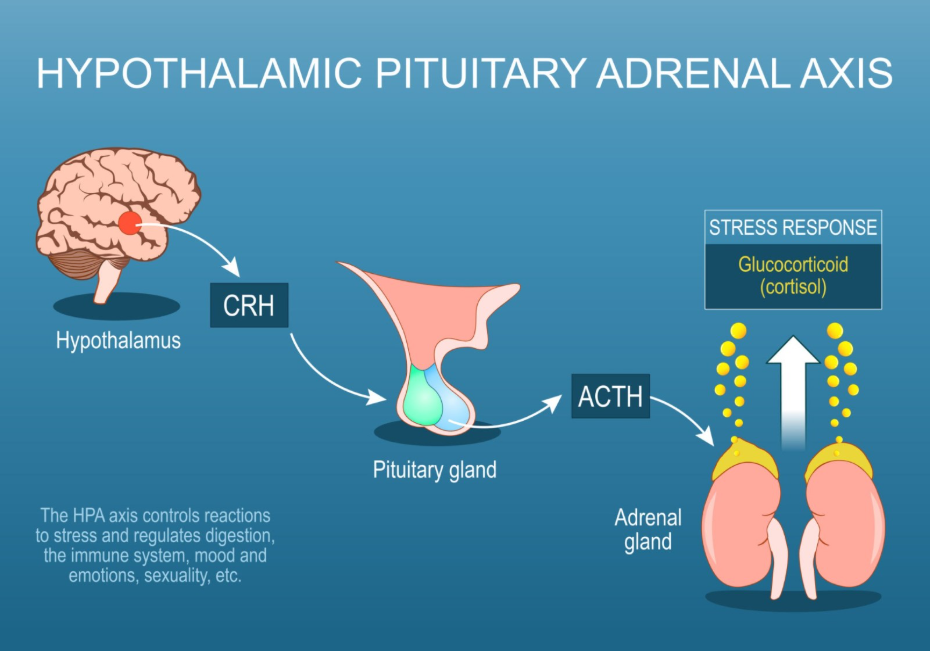
The progression from anxiety to depression is rooted in the body’s autonomic nervous system, where the prolonged activation of the stress response can lead to a biological state of “burnout.” In the United Kingdom, clinical frameworks explain that when the adrenal glands consistently produce high levels of cortisol to manage anxiety, the brain’s emotional regulation centres may eventually become desensitised or exhausted. The NHS states that it is very common for people to have both depression and anxiety at the same time.
This transition occurs because the same neural pathways involved in threat detection, such as the amygdala, also influence the mood-regulating centres in the hippocampus. When the system is overtaxed by persistent worry, the ability to process positive emotions and maintain energy levels is significantly reduced. In the UK, this professional framework provides a stable foundation for the health journey by identifying that these sensations are biological realities. By utilised these integrated pathways, the healthcare system ensures that every person’s profile is supported through evidence-based understanding. This coordinated effort between primary care and specialists provides a secure environment for building emotional resilience.
Identifying Overlapping and Evolving Symptoms
As anxiety begins to lead toward a depressive episode, an individual may notice a shift from “high-energy” symptoms, like panic or restlessness, to “low-energy” symptoms, such as withdrawal and apathy. In the United Kingdom, healthcare professionals categorise these evolving markers to help identify the most effective integrated management plan before a full depressive episode develops. NICE clinical guidelines for common mental health problems indicate that a thorough assessment should identify the presence of both anxiety and depression to ensure appropriate care.
| Symptom Feature | Primary Anxiety Manifestation | Transition Toward Depression |
| Physical Energy | Feeling “wired,” shaky, or restless. | Feeling physically heavy, slow, or exhausted. |
| Sleep Patterns | Difficulty falling asleep due to worry. | Oversleeping or early morning waking with low mood. |
| Social Interaction | Fear of social judgment or panic. | Loss of interest in socialising and isolation. |
| Cognitive State | Hyper-focus on future perceived threats. | Feeling that the future is hopeless or “flat.” |
| Emotional Response | Heightened irritability and alertness. | Pervasive sadness or inability to feel pleasure. |
In the UK, these challenges are managed through integrated care plans that prioritise a person-centred approach. Identifying that the “exhaustion” following a period of high anxiety is a clinical indicator can help individuals access support earlier. This professional oversight is essential for providing a safe and accurate understanding of the individual’s functional capability. By building a robust evidence base through clinical review, the multidisciplinary team can provide more effective strategies for long-term health.
Neurotransmitter Depletion and Mood Stability
The regulation of neurotransmitters such as serotonin and dopamine is vital for both managing anxiety and maintaining a stable mood, and the chronic strain of worry can deplete these essential chemicals. In the United Kingdom, healthcare professionals focus on how the brain’s chemical messengers facilitate communication between neurons to maintain emotional balance. The GOV.UK health pages provide clinical profiles indicating that the monitoring of social and cognitive challenges is a priority for ensuring integrated support.
When the brain is constantly using its resources to manage the “volume” of anxiety, there is often less available to support the reward and motivation pathways. This chemical depletion can manifest as the loss of interest and persistent low mood found in depression. In the UK, the focus is on providing a stable foundation where management strategies are designed to support these biological pathways. Identifying these underlying drivers allows for more targeted help that addresses the biological cause of distress. By utilised these professional frameworks, the UK system provides a life-long framework of support that adapts to the person’s needs.
The Role of Avoidance and Social Isolation
Avoidance is a common coping mechanism for anxiety, but when used long-term, it can lead to social isolation and a lack of positive reinforcement, which are major environmental triggers for depression. In the United Kingdom, specialists recognise that the “safety behaviours” used to manage anxiety, such as staying at home or avoiding social gatherings, can inadvertently shrink an individual’s world.
This reduced social engagement prevents the brain from receiving the natural “mood boosts” that come from connection and achievement. Over time, the lack of stimulation and connection can result in a depressive episode. In the UK, this integrated care model ensures that the adult’s or child’s emotional potential is supported within their social context. This professional oversight is essential for providing a safe and accurate understanding of the individual’s emotional health. By acknowledged these biological and social differences, the system provides a more supportive framework for managing the person’s unique profile safely.
Integrated NHS Management and Support
Management strategies for individuals whose anxiety is leading to depression in the United Kingdom focus on a coordinated approach that addresses both the overactive stress response and the emerging low mood. The NHS prioritises talking therapies, such as Cognitive Behavioural Therapy, which can be tailored to help individuals manage both their worries and their motivation levels.
Commonly utilised integrated strategies in the UK include:
- Adapted Talking Therapies: Addressing the “vicious cycle” of how anxiety leads to withdrawal and subsequently to depression.
- Behavioural Activation: Gradually re-introducing meaningful activities to boost mood and reduce avoidance.
- Relaxation Techniques: Practising mindfulness to lower the body’s physical stress response and manage intrusive thoughts.
- Sleep Hygiene: Establishing a structured routine to support the restorative rest needed for neurochemical recovery.
- Social Prescribing: Connecting with community groups to overcome the isolation caused by anxiety-driven avoidance.
In the UK, identifying these indicators early is vital for preventing the emotional exhaustion that can accompany complex mental health challenges. By utilised these professional frameworks, the healthcare system provides a secure environment for building professional and personal confidence. These strategies aim to work with the individual’s biology to restore a sense of calm and purpose.
Accessing Integrated NHS Support Pathways
The pathway for managing co-occurring anxiety and depression in the United Kingdom is a coordinated process involving GPs and mental health specialists through services like NHS Talking Therapies. This journey ensures that every individual receives a thorough review of their history and current environment to build a bespoke management plan.
The UK integrated support pathway involves:
- Initial GP Consultation: Discussing how symptoms have changed from worry to low mood over time.
- Clinical Assessment: Undergoing a formal review to identify the primary drivers and severity of both conditions.
- Referral to Therapy: Accessing evidence-based talking therapies that are tailored to manage complex or evolving profiles.
- Integrated Care Planning: Co-ordinating support between the health service and any necessary workplace or educational adjustments.
- Regular Monitoring: Scheduled reviews to ensure that management strategies remain effective and safe as symptoms fluctuate.
In the UK, the focus is on providing a stable foundation for the individual to move forward with self-understanding. The NHS ensures that adults and children have a consistent point of contact for their health needs while they navigate their lives. This integrated approach ensures that the person’s unique way of functioning is respected within their home and work environment. By utilised these integrated pathways, the healthcare system provides a secure environment for building long-term mental wellbeing.
Conclusion
Persistent anxiety can lead to depressive episodes due to the biological exhaustion of the stress response and the impact of social avoidance within the United Kingdom’s healthcare framework. The NHS and professional bodies provide a robust system of multidisciplinary assessments and evidence-based therapies to help individuals manage these evolving profiles effectively. By focusing on both the biological roots of stress and the need for supportive environments, the system promotes the highest possible level of independence. Following a coordinated management plan with the help of medical and psychological experts ensures that unique adult and paediatric needs are addressed holistically.
Why does my anxiety feel like it is turning into depression?
Long-term anxiety can exhaust your nervous system, leading to the low energy and hopelessness that characterise depression.
Can I prevent depression if I already have anxiety?
Yes; early intervention in the UK focusing on pacing, relaxation, and reducing avoidance can help protect your emotional resources.
Is the treatment the same for both?
While there is overlap, the clinical team will add strategies like “behavioural activation” to specifically target the low mood.
Why do I feel so tired after a panic attack?
A panic attack is a massive surge of adrenaline; once it passes, your body enters a natural recovery phase of deep fatigue.
Does exercise help if I feel both anxious and low?
Yes; physical activity is an evidence-based way to burn off anxious energy and boost mood-regulating chemicals like endorphins.
What is “comorbidity”?
It is the clinical term used when a person has more than one distinct health condition, such as anxiety and depression, at the same time.
Who should I talk to first if my symptoms are changing?
The first point of contact in the United Kingdom is usually your GP to discuss your health and explore updated support options.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the link between anxiety and depression, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in multiple clinical specialties including cardiology, emergency medicine, and psychiatry. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
