Pregnancy and childbirth can trigger depression or anxiety because of the profound biological shifts in hormone levels, significant changes to the autonomic nervous system, and the physical exhaustion associated with the transition to parenthood. In the United Kingdom, these conditions are recognised as perinatal mental health challenges. By utilising integrated NHS support pathways, individuals can access evidence-based clinical care to restore their functional and emotional stability.
What We’ll Discuss in This Article
- The biological relationship between hormonal shifts and mood regulation.
- Distinguishing between the baby blues and perinatal mental health conditions.
- How the stress response system adapts during pregnancy and postpartum.
- Identifying physical and cognitive markers of perinatal anxiety and depression.
- The role of integrated NHS specialist teams in supporting new parents.
- Accessing professional clinical reviews and evidence-based management.
Biological Foundations of Perinatal Mental Health
Pregnancy and childbirth trigger significant neurochemical and hormonal changes, such as rapid fluctuations in oestrogen and progesterone, which can directly influence the brain regions responsible for emotional regulation and the stress response. In the United Kingdom, healthcare professionals identify that these biological shifts can impact the sensitivity of the nervous system, potentially leading to persistent low mood or anxiety. The NHS states that many women feel a bit down, tearful or anxious in the first week after giving birth, often called the baby blues.
While temporary emotional shifts are common, persistent symptoms suggest a deeper biological dysregulation. In the UK, this professional framework provides a stable foundation for the health journey by identifying that perinatal health is rooted in physiological transitions. By utilised these integrated pathways, the healthcare system ensures that every person’s profile is supported through evidence-based understanding. This coordinated effort prioritises the safety of the individual and their family within a validated medical environment.
Distinguishing Clinical Conditions from Baby Blues
Clinical perinatal depression or anxiety is distinguished from the baby blues by the severity and persistence of symptoms, which often interfere with an individual’s ability to perform daily functional tasks or care for their infant. In the United Kingdom, clinicians use standardised assessments to monitor whether the autonomic nervous system is achieving homeostasis or remains in a state of chronic hyper-arousal. NICE clinical guidelines for antenatal and postnatal mental health indicate that early identification and evidence-based intervention are essential for long-term family wellbeing.
| Feature | Baby Blues | Perinatal Depression or Anxiety |
| Onset | Usually 3 to 10 days after birth. | Can start during pregnancy or anytime in the first year. |
| Duration | Typically resolves within a few days. | Persistent for several weeks or months. |
| Intensity | Mild tearfulness and irritability. | Overwhelming sadness, worry, or lack of interest. |
| Biological Impact | Minor fatigue and mood shifts. | Significant disruption to sleep, appetite, and energy. |
| Functional Effect | Daily tasks are usually maintained. | Interference with self-care and infant care. |
In the UK, these biological markers are managed through integrated care plans that prioritise a person-centred approach. Identifying that physical signs like a racing heart or leaden fatigue are biological responses helps the multidisciplinary team select the most effective management strategy. This professional oversight is essential for providing a safe and accurate understanding of the individual’s health needs. By building a robust evidence base through clinical review, the healthcare system provides a secure environment for building long-term health.
The Stress Response and Physical Exhaustion
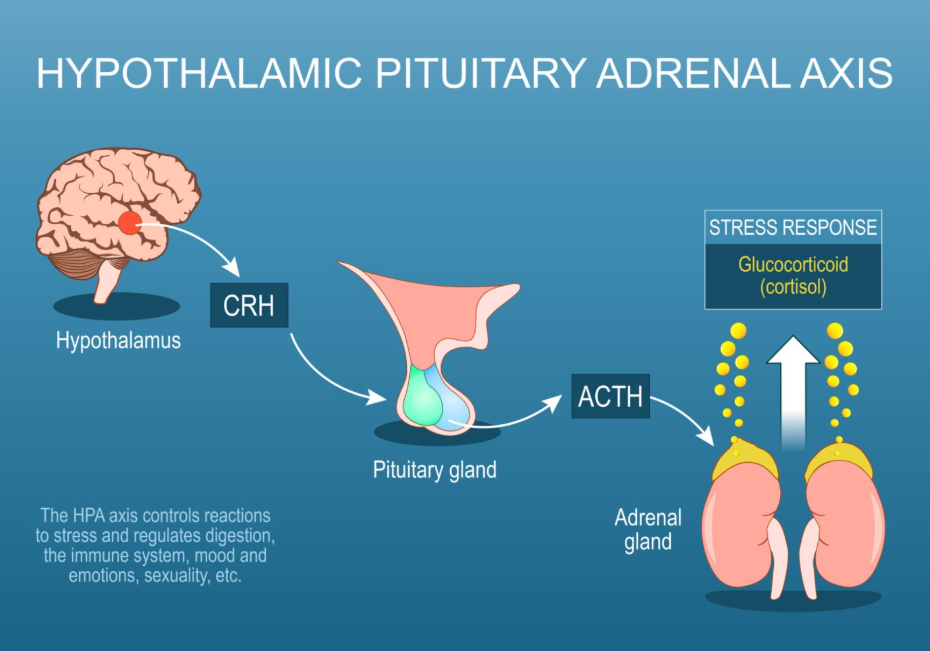
The physical demands of childbirth and infant care can maintain the body in a state of chronic sympathetic nervous system activation, which depletes metabolic resources and increases the risk of developing clinical anxiety or depression. In the United Kingdom, specialists recognise that sleep deprivation is a major biological stressor that can impair the prefrontal cortex’s ability to regulate the amygdala’s emotional signals. The GOV.UK health pages provide clinical profiles indicating that the monitoring of social and cognitive challenges is a priority for ensuring integrated support during the perinatal period.
By addressing physical exhaustion alongside psychological symptoms, the healthcare system promotes a more holistic recovery. In the UK, the focus is on providing a stable foundation where the individual’s environment is reviewed alongside their metabolic health. Identifying these underlying drivers allows for more targeted help that addresses the actual biological cause of distress. By utilised these professional frameworks, the UK system provides a life-long framework of support that adapts to the person’s needs.
Identifying Markers of Perinatal Distress
Identifying the markers of perinatal distress involves looking for a combination of physical and cognitive indicators that suggest the nervous system is struggling to adapt to the biological and social changes of parenthood. In the United Kingdom, healthcare professionals focus on these signs during routine health visitor and midwife appointments to ensure that individuals receive timely support.
Common markers identified in the UK include:
- Persistent Hyper-vigilance: A constant state of alertness or worry regarding the infant’s safety.
- Sleep Disruption: Inability to sleep even when the infant is sleeping and the opportunity is available.
- Cognitive Brain Fog: Significant difficulty in concentrating, making decisions, or retaining information.
- Physical Tension: Chronic bracing in the neck and shoulders or persistent headaches.
- Appetite Shifts: Notable loss of interest in food or significant changes in eating patterns.
- Emotional Withdrawal: Feeling detached from the infant or lacking interest in previously enjoyed activities.
In the UK, identifying these indicators early is vital for preventing the functional decline that often accompanies untreated perinatal conditions. The integrated support framework encourages a strengths-based approach, focusing on what the individual needs to remain healthy. By utilised these professional frameworks, the healthcare system provides a secure environment for building parental confidence. These strategies aim to work with the individual’s biology to restore a sense of calm.
Accessing Integrated NHS Support Pathways
The pathway for managing perinatal mental health in the United Kingdom is a coordinated process involving midwives, health visitors, GPs, and specialist perinatal mental health teams. This journey ensures that every individual receives a thorough review of their history and current environment to build a bespoke recovery plan that supports their wellness and their relationship with their child.
The UK integrated support pathway involves:
- Routine Screening: Regular health reviews during pregnancy and the first year after birth.
- GP Consultation: Discussing physical and emotional symptoms for a clinical review.
- Specialist Teams: Accessing multidisciplinary care from psychiatrists and mental health nurses.
- Talking Therapies: Utilising evidence-based support such as Cognitive Behavioural Therapy (CBT).
- Physical Health Review: Performing blood tests to rule out biological causes like thyroid issues.
- Peer Support: Connecting with other parents to reduce isolation and biological stress.
In the UK, the focus is on providing a stable foundation for the individual to move forward with self-understanding. The NHS ensures that parents have a consistent point of contact for their health needs while they navigate their lives. By utilised these integrated pathways, the healthcare system provides a secure environment for building long-term mental wellbeing across the UK population. These strategies aim to work with the individual’s biology to restore a sense of calm and purpose.
Conclusion
Pregnancy and childbirth are significant biological events that can trigger depression or anxiety through complex hormonal shifts and physical strain within the United Kingdom’s healthcare framework. The NHS and professional bodies provide a robust system of multidisciplinary assessments and specialist care to help parents achieve stability and resilience. By focusing on both the biological roots of symptoms and the need for supportive environments, the system promotes the highest possible level of health for the whole family. Following a coordinated management plan with the help of medical and psychological experts ensures that unique adult and paediatric needs are addressed holistically.
Is it my fault if I feel this way after having a baby?
No; perinatal mental health conditions are biological health factors caused by hormonal shifts and physical stress, not personal failings.
How can I tell if I have more than the “baby blues”?
If your feelings of sadness or anxiety last longer than two weeks or interfere with your daily life, you should speak to a healthcare professional.
Can men experience perinatal depression or anxiety?
Yes; partners can also experience significant mental health challenges due to the lifestyle changes and stress associated with a new infant.
Will I have to take medication if I am breastfeeding?
Many management options exist, including talking therapies; if medication is required, UK clinicians will discuss the safest options for you and your baby.
How does sleep deprivation affect my mood?
Sleep loss disrupts your brain’s ability to regulate emotions, which can lead to increased irritability and a higher risk of depression.
Will the NHS take my baby away if I ask for help?
No; the goal of the NHS is to support you and your baby to stay together safely by providing the clinical care you need to recover.
Who should I talk to first if I am worried about my health?
The first point of contact in the United Kingdom is usually your midwife, health visitor, or GP to discuss your health and explore pathways.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding perinatal mental health, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in multiple clinical specialties including emergency care, general surgery, and medical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
