Cerebral palsy affects speech by disrupting the neurological control of the muscles required for breathing, vocalising, and articulating sounds, often leading to challenges with clarity and volume. In the United Kingdom, these communication difficulties are managed by multidisciplinary teams within the NHS to help individuals maximise their functional expression. While not everyone with the condition experiences speech issues, many benefit from early, integrated therapy.
What We’ll Discuss in This Article
- The biological impact of muscle dyscoordination on speech production.
- Understanding dysarthria and its different manifestations in the UK.
- How breathing and breath control influence vocal volume and rhythm.
- The role of Augmentative and Alternative Communication (AAC) systems.
- Managing associated challenges such as swallowing and saliva control.
- Accessing specialist NHS speech and language therapy services.
Neurological Impact on Speech Muscle Coordination
Cerebral palsy affects speech by interfering with the brain ability to coordinate the complex movements of the tongue, lips, jaw, and vocal folds needed for clear communication. Because the condition is a motor disorder, the same neurological injury that affects walking or reaching also impacts the fine motor skills used for talking. The NHS states that cerebral palsy can affect a person’s ability to communicate, and some people may have difficulty speaking or may not be able to speak at all.
In the United Kingdom, clinicians refer to speech difficulties caused by muscle weakness or stiffness as dysarthria. When the motor control centres of the brain are damaged, the signals sent to the facial muscles may be delayed, weak, or uncoordinated. This can result in speech that sounds slurred, slow, or difficult to understand. The severity of the impact depends on which part of the brain was injured; for example, damage to the cerebellum may cause shaky or rhythmic speech patterns. Specialist speech and language therapists (SLTs) in the UK perform detailed assessments to identify which specific muscle groups are most affected. By understanding the neurological origin of the speech challenge, the healthcare team can provide targeted exercises to improve the precision of these movements.
Types of Speech Challenges: Dysarthria and Dyspraxia
The way cerebral palsy affects speech is often categorised into different types of dysarthria, which reflect the underlying movement disorder present in the individual’s body. In the United Kingdom, identifying the specific type of speech impairment is essential for selecting the most effective therapeutic strategies and communication aids. NICE clinical guidelines for cerebral palsy indicate that speech and language assessments should consider the individual’s motor profile, including spasticity or dyskinesia.
| Type of Impairment | Primary Speech Characteristics | Typical Muscle Movement |
| Spastic Dysarthria | Harsh or strained voice; slow rate. | Muscles are stiff and tight. |
| Dyskinetic Dysarthria | Variable volume; sudden interruptions. | Involuntary, uncontrolled motions. |
| Ataxic Dysarthria | Shaky voice; slurred articulation. | Poor balance and coordination. |
| Verbal Dyspraxia | Difficulty planning speech sounds. | Poor sequencing of movements. |
Individuals with spasticity may have a voice that sounds tight because the muscles of the larynx are overactive. Those with dyskinetic cerebral palsy may experience sudden changes in pitch or volume because their breathing and vocal muscles move involuntarily. Some individuals may also have verbal dyspraxia, where the brain struggles to plan the sequence of movements needed to say a word, even if the muscles themselves are strong. In the UK, the SLT works to help the individual find the most reliable way to produce sounds. Integrated support ensures that the person’s communication style is understood by their family and carers, reducing frustration and supporting social participation.
Breathing and Breath Control for Vocalisation
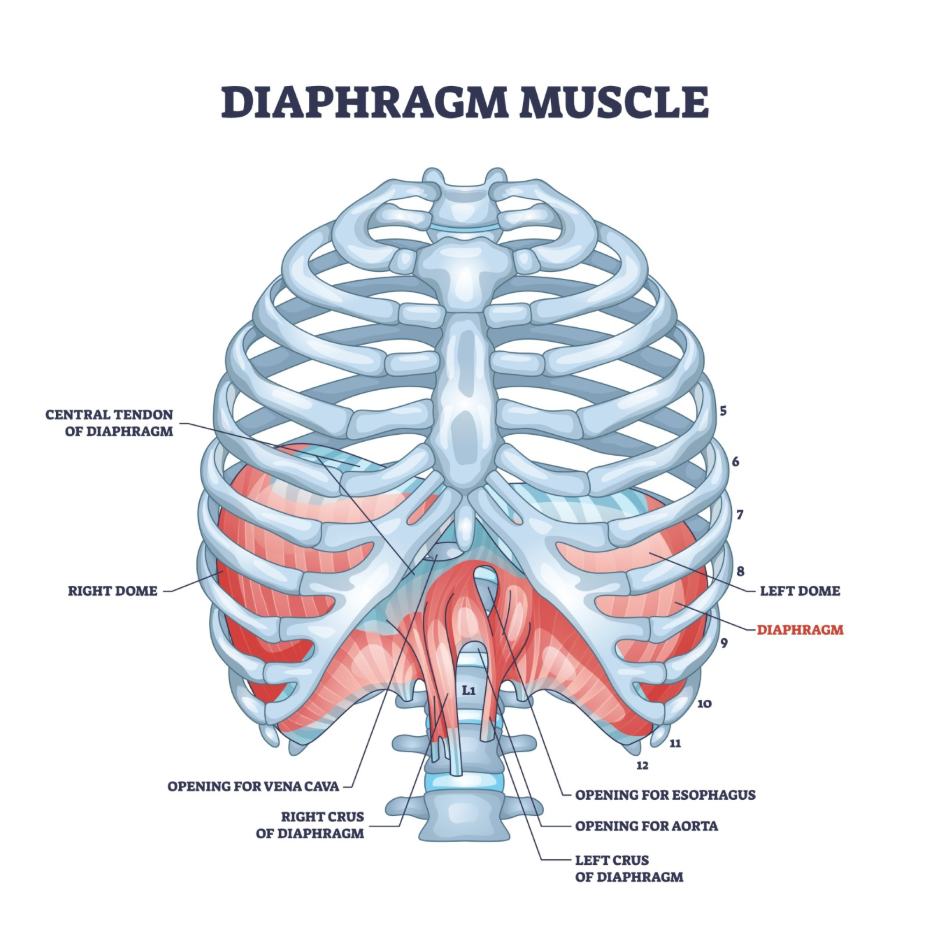
Speech production relies on a steady and controlled flow of air from the lungs, and cerebral palsy can affect movement in a way that makes this breath control challenging to maintain. If the muscles used for breathing (such as the diaphragm and intercostals) are stiff or weak, the person may struggle to produce enough air pressure to speak loudly or to finish a long sentence in one breath.
In the United Kingdom, SLTs often work on “respiratory support” as a foundation for speech therapy. Challenges may include:
- Short Phrases: Only being able to say one or two words before needing to take another breath.
- Quiet Volume: A voice that is difficult to hear in noisy environments because of low air pressure.
- Irregular Rhythm: Speech that sounds chopped up because breathing is not synchronised with talking.
- Vocal Fatigue: Feeling physically tired after speaking for a short period.
Improving breath control helps to provide a more stable power source for the voice. In the UK healthcare system, therapists use practical exercises to help individuals coordinate their breathing with the start of a sentence. For some, learning to use shorter sentences or taking frequent pauses can make their speech clearer and less exhausting. By addressing the respiratory aspect of communication, the NHS support team helps individuals communicate more effectively in their daily lives, whether at home, in school, or at work.
Augmentative and Alternative Communication (AAC)
When cerebral palsy affects speech so significantly that verbal communication is difficult to understand, the United Kingdom provides access to Augmentative and Alternative Communication (AAC) systems to ensure the individual can express themselves fully. AAC encompasses a wide range of tools, from simple picture boards to advanced computer systems that generate speech. The GOV.UK health pages provide clinical profiles indicating that the provision of communication aids is a key part of the integrated social and health support for neurological conditions.
Common AAC options in the UK include:
- Low-Tech Systems: Symbol boards, books, or cards that a person points to.
- Mid-Tech Systems: Simple electronic devices that play pre-recorded messages.
- High-Tech Systems: Eye-gaze technology or tablets with specialist software that converts text or symbols to speech.
- Signing and Gestures: Using manual signs to supplement or replace spoken words.
The choice of AAC depends on the individual’s physical abilities, such as their hand coordination or eye movement. In the UK, specialist AAC hubs provide assessments to find the most suitable technology for each person. These tools are integrated into the person’s Education, Health and Care (EHC) plan to ensure they can be used effectively in school or college. AAC does not stop a person from learning to talk; instead, it provides a reliable way to communicate while they work on their physical speech skills. This integrated approach prioritises the individual’s right to be heard and understood in all areas of their life.
Managing Swallowing and Saliva Challenges
Because the same muscles are used for both speaking and eating, cerebral palsy often affects swallowing (dysphagia) and saliva management alongside speech. In the United Kingdom, SLTs are responsible for assessing and managing these oral-motor challenges to ensure the individual can eat and drink safely while maintaining their dignity.
Challenges managed by the NHS include:
- Drooling: Difficulty swallowing saliva regularly, which can impact social confidence and skin health.
- Swallowing Difficulties: Problems moving food or liquid safely from the mouth to the stomach.
- Chewing Issues: Weakness in the jaw muscles making it hard to manage different food textures.
- Coughing During Meals: A sign that food or drink may be entering the airway.
In the UK, the SLT may recommend specific exercises to strengthen the lips and tongue or suggest changes to food textures to make swallowing easier. Saliva management can sometimes be assisted with medications or specialist therapy to encourage more frequent swallowing. Addressing these oral-motor needs is a vital part of the holistic care provided for cerebral palsy. It ensures that the person remains healthy and comfortable, which in turn provides a better physical foundation for their communication efforts. The NHS provides consistent monitoring to ensure that swallowing remains safe as the individual grows or their physical needs change.
Accessing Integrated NHS Speech and Language Therapy
The United Kingdom provides a comprehensive framework of integrated support to help individuals with cerebral palsy manage their communication and swallowing needs throughout their lives. This involves a coordinated effort between health, education, and social services to provide a consistent safety net.
The UK support framework involves:
- Early Intervention: Referral to an SLT as soon as communication or feeding concerns are identified in infancy.
- School-Based Support: Integrating communication goals into the classroom environment.
- Regular Reviews: Scheduled assessments to update therapy goals and communication equipment.
- Adult Services: Transitioning to adult SLT teams to support communication in work and community settings.
In the UK, the SLT works within a multidisciplinary team that includes physiotherapists and occupational therapists. This ensures that the person’s posture which is essential for good breathing and speech is supported correctly. Accessing these services through a GP or hospital consultant ensures that the care is evidence-based and aligned with national standards. By providing this continuous support, the NHS aims to empower every individual with cerebral palsy to achieve their greatest possible level of communicative independence.
Conclusion
Cerebral palsy affects speech by disrupting the motor control of the muscles used for articulation, breathing, and vocalisation. In the UK, the NHS manages these challenges through specialist speech and language therapy, focusing on improving muscle coordination and providing communication aids like AAC where needed. While speech may be slurred or quiet due to dysarthria, integrated therapy helps individuals find alternative ways to express themselves. Managing associated issues like swallowing and saliva control is also a core part of the care pathway. Following a structured multidisciplinary plan ensures the best possible outcomes for social and functional communication. The UK healthcare system provides a life-long framework of support for these neurological challenges. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does every child with cerebral palsy have speech problems?
No; many children with the condition have clear speech, although they may still benefit from support with other communication skills.
Can a speech therapist help with drooling?
Yes; in the UK, speech and language therapists provide exercises and strategies to help manage saliva and improve lip closure.
Will using a communication aid stop my child from learning to speak?
No; research shows that AAC often supports language development and can reduce the frustration that might hinder speech progress.
What is eye-gaze technology?
It is a high-tech communication system used in the UK that allows a person to control a computer and “speak” using only their eye movements.
Does cerebral palsy affect the ability to understand language?
Most people with cerebral palsy understand language well, although some may have associated learning needs that affect their processing.
Why does my child’s voice sound strained?
This is often due to spasticity in the muscles of the voice box, which makes it difficult to produce a relaxed, smooth sound.
Can adults with cerebral palsy still get speech therapy?
Yes; the NHS provides adult speech and language therapy services to help maintain communication skills and manage any new challenges.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding how cerebral palsy affects speech, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in general surgery, cardiology, and emergency medicine. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
