A brain tumour is a growth of cells in the brain that multiplies in an abnormal, uncontrollable way. These growths can originate within the brain tissue itself or spread to the brain from other parts of the body. Because the brain is enclosed within the rigid structure of the skull, any extra growth can create pressure or interfere with the normal functioning of the central nervous system. In the United Kingdom, healthcare professionals categorise these tumours based on their cellular characteristics and their potential to grow or spread. While the word tumour can be concerning, it is important to note that many growths are non-cancerous and may remain stable for long periods. The UK healthcare system uses a structured approach to identify and monitor these growths, ensuring that patients receive care aligned with national clinical standards. Understanding the fundamental nature of these cell clusters is the first step in navigating the diagnostic and management process. By adhering to evidence-based protocols established by the NHS and NICE, clinicians aim to manage the symptoms caused by the growth while preserving as much neurological function as possible.
What We’ll Discuss in This Article
- The biological difference between primary and secondary tumours.
- How clinicians distinguish between low-grade and high-grade growths.
- Common symptoms and how they relate to the location of the growth.
- The diagnostic process used in the UK, including imaging and biopsies.
- An overview of management options such as surgery and monitoring.
- UK clinical pathways for long-term care and patient support.
Primary and Secondary Brain Tumours
Brain tumours are fundamentally divided into primary tumours, which start in the brain, and secondary tumours, which are formed by cells that have travelled to the brain from another part of the body. Primary tumours develop from the various cells that make up the brain and its protective coverings, such as glial cells or meningeal tissue. The NHS states that a brain tumour is a growth of cells in the brain that multiplies in an abnormal, uncontrollable way.
Secondary tumours, also known as brain metastases, occur when cancer cells from organs like the lungs or breasts spread through the bloodstream to the brain. In the United Kingdom, identifying whether a tumour is primary or secondary is a priority because the origin of the cells determines the management strategy. Primary tumours are often named after the specific cell type they involve, such as gliomas or meningiomas. Understanding this distinction helps clinical teams decide whether to focus solely on the brain or to investigate other areas of the body to ensure a comprehensive care plan.
Grading and Cellular Behaviour
Clinicians in the UK use a grading system to describe how quickly a brain tumour is likely to grow and how likely it is to spread into the surrounding tissue. This grading is usually determined by looking at the tumour cells under a microscope to see how abnormal they appear compared to healthy cells. NICE clinical guidelines for brain tumours and suspensions of the central nervous system indicate that tumours are graded from 1 to 4 to help determine the most appropriate management pathway.
Low-grade tumours (grades 1 and 2) are typically slow-growing and less likely to spread, often referred to as non-cancerous or benign. High-grade tumours (grades 3 and 4) grow more rapidly and are considered cancerous or malignant.
| Tumour Grade | Growth Rate | Description |
| Grade 1 | Very slow | Non-cancerous; often curable with surgery. |
| Grade 2 | Slow | May recur after treatment or progress to higher grade. |
| Grade 3 | Fast | Malignant; cells look quite different from normal cells. |
| Grade 4 | Very fast | Most aggressive; requires intensive management. |
This grading system allows UK medical teams to predict the behaviour of the growth and provide patients with a clearer understanding of the necessary follow-up. It also ensures that resources are directed appropriately toward those with more aggressive cell types.
Symptoms and the Impact of Location
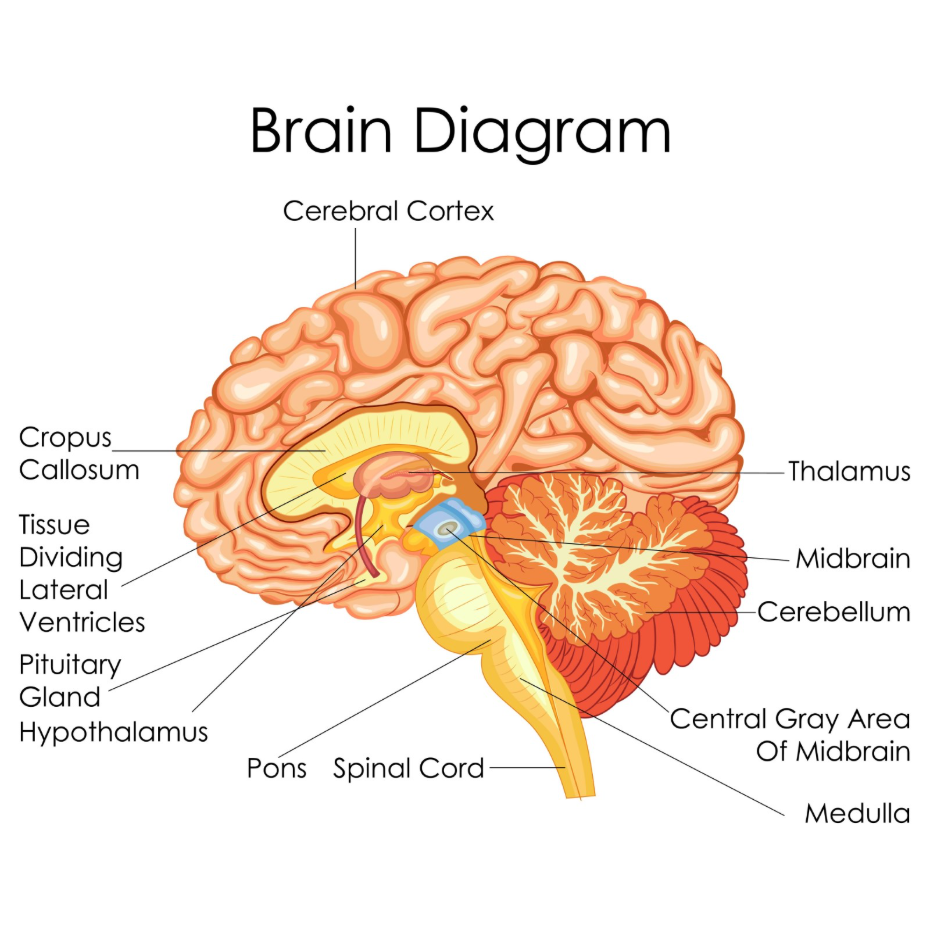
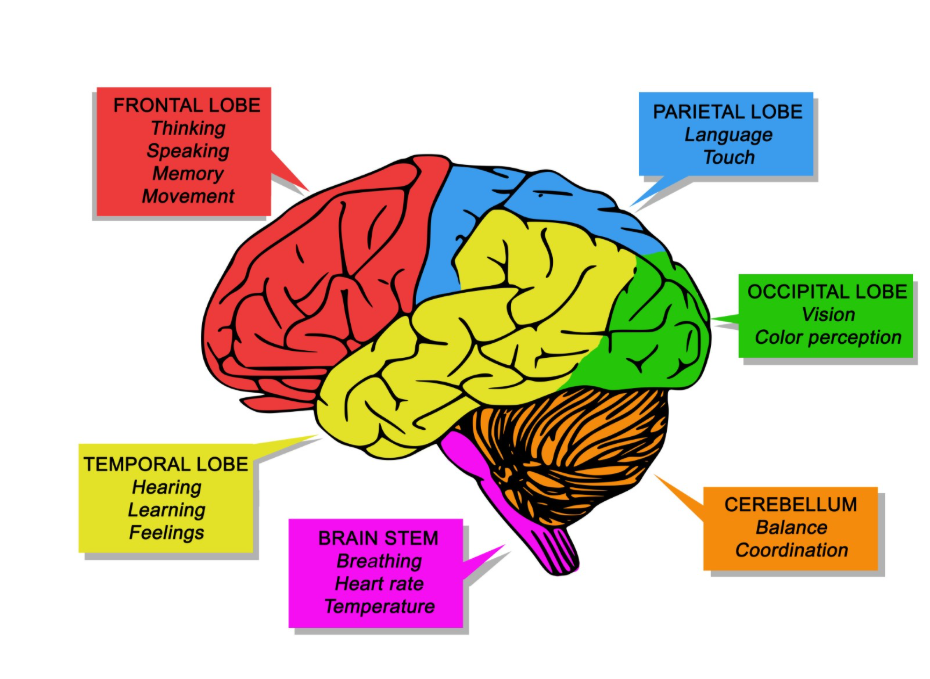
The symptoms caused by a brain tumour depend largely on its size and which part of the brain is being affected by the growth or the surrounding swelling. Because different areas of the brain control different functions, a tumour in the frontal lobe might affect personality, while one in the occipital lobe might affect vision.
Common general symptoms include persistent headaches that are often worse in the morning, seizures, or feelings of nausea. Some individuals may experience subtle changes, such as weakness on one side of the body or difficulty with coordination and balance. In the United Kingdom, if symptoms are persistent or unusual, clinicians use neurological examinations to check for signs of pressure or functional loss. It is important to remember that many of these symptoms are also caused by much less serious conditions, such as migraines or infections. However, professional evaluation is necessary to determine the underlying cause and ensure that any structural issues within the skull are identified early.
The UK Diagnostic Pathway
The process of identifying a brain tumour in the UK usually begins with a referral for a specialised scan, such as an MRI or CT, to create a detailed picture of the internal structures of the brain. An MRI scan is particularly useful as it uses strong magnets to produce high-resolution images that can show the exact size, shape, and location of a growth. The GOV.UK health pages provide information on the standard procedures for diagnostic imaging to ensure consistency across the NHS.

If a scan reveals a suspicious area, a specialist known as a neurosurgeon may perform a biopsy. This involves taking a small sample of the tissue so that it can be examined in a laboratory to confirm the grade and type of the cells. In some cases, if the tumour is in an accessible location, the entire growth might be removed during surgery rather than just taking a biopsy. This diagnostic sequence ensures that the management plan is based on accurate biological data rather than just visual appearance. By following these national protocols, the UK healthcare system minimises diagnostic uncertainty and provides a clear route toward treatment.
Management and Long-Term Care
Management for a brain tumour in the United Kingdom is highly personalised and may include surgery, monitoring, or other clinical interventions depending on the tumour’s grade and location. For slow-growing, low-grade tumours that are not causing symptoms, a clinician might recommend “watch and wait,” which involves regular scans to see if the growth changes over time.
If the tumour is causing pressure or is high-grade, surgery is often the first step to remove as much of the growth as possible. Other management tools may be used to target any remaining cells or to shrink the tumour before surgery. Throughout this process, patients are supported by a Multidisciplinary Team (MDT), which includes surgeons, oncologists, and specialist nurses. This team works together to manage side effects, such as swelling or seizures, and to support the patient’s overall quality of life. Long-term care often involves rehabilitation, such as physiotherapy or speech therapy, to help the brain recover after treatment. The UK pathway is designed to be comprehensive, addressing both the physical growth and the functional needs of the individual.
Conclusion
A brain tumour is an abnormal growth of cells within the brain that requires professional evaluation and management. In the UK, these growths are graded and categorised to determine the best course of care, with the NHS providing a structured pathway from imaging to long-term support. While some tumours are aggressive, many are slow-growing and can be managed effectively for many years. Maintaining communication with your clinical team and attending all scheduled follow-ups is essential for managing the condition. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Are all brain tumours cancerous?
No, many brain tumours are low-grade and non-cancerous, meaning they grow slowly and do not spread to other parts of the body.
Can a brain tumour be caused by a head injury?
There is currently no scientific evidence to suggest that a bump or injury to the head causes a brain tumour to develop.
How long does it take to get a diagnosis in the UK?
Diagnostic timelines vary, but the NHS aims to see patients with suspected brain tumours urgently for imaging and specialist review.
Is surgery always necessary?
No, some tumours are managed with regular monitoring or other non-surgical methods if they are not causing symptoms or are in a difficult location.
Can children get brain tumours?
Yes, brain tumours can occur at any age, and the UK has specialised paediatric units to manage the specific needs of younger patients.
Do brain tumours run in families?
Most brain tumours are not hereditary, although a very small number are linked to specific genetic conditions.
Can I drive if I have a brain tumour?
In the UK, you must inform the DVLA of a brain tumour diagnosis, as the condition or its treatment may affect your ability to drive safely.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding brain tumours, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in emergency care, surgery, and clinical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
