A glioma is a common type of primary brain tumour that originates in the glial cells, which are the supportive tissues that surround and nourish neurons in the central nervous system. These tumours are categorised based on the specific type of glial cell involved and are graded according to how quickly the cells are likely to grow and spread into surrounding brain tissue. In the United Kingdom, healthcare professionals use advanced diagnostic imaging and molecular testing to identify gliomas and determine the most appropriate management pathway for each patient. While the discovery of a brain tumour is a significant event, understanding the biological nature of glial cells and the standardised grading system used by the NHS provides a clear framework for navigating the clinical journey. By following evidence-based protocols established by NICE, medical teams aim to manage the condition while prioritising the preservation of neurological function and quality of life. This article explores the different varieties of gliomas and the clinical processes involved in their assessment within the UK healthcare system.
What We’ll Discuss in This Article
- The biological role of glial cells in the central nervous system.
- The primary types of gliomas including astrocytomas and ependymomas.
- How the World Health Organization (WHO) grading system is applied.
- Common symptoms associated with glial cell tumours.
- The diagnostic process using MRI scans and biopsies in the UK.
- Integrated management pathways for low-grade and high-grade gliomas.
The Biological Origin of Gliomas
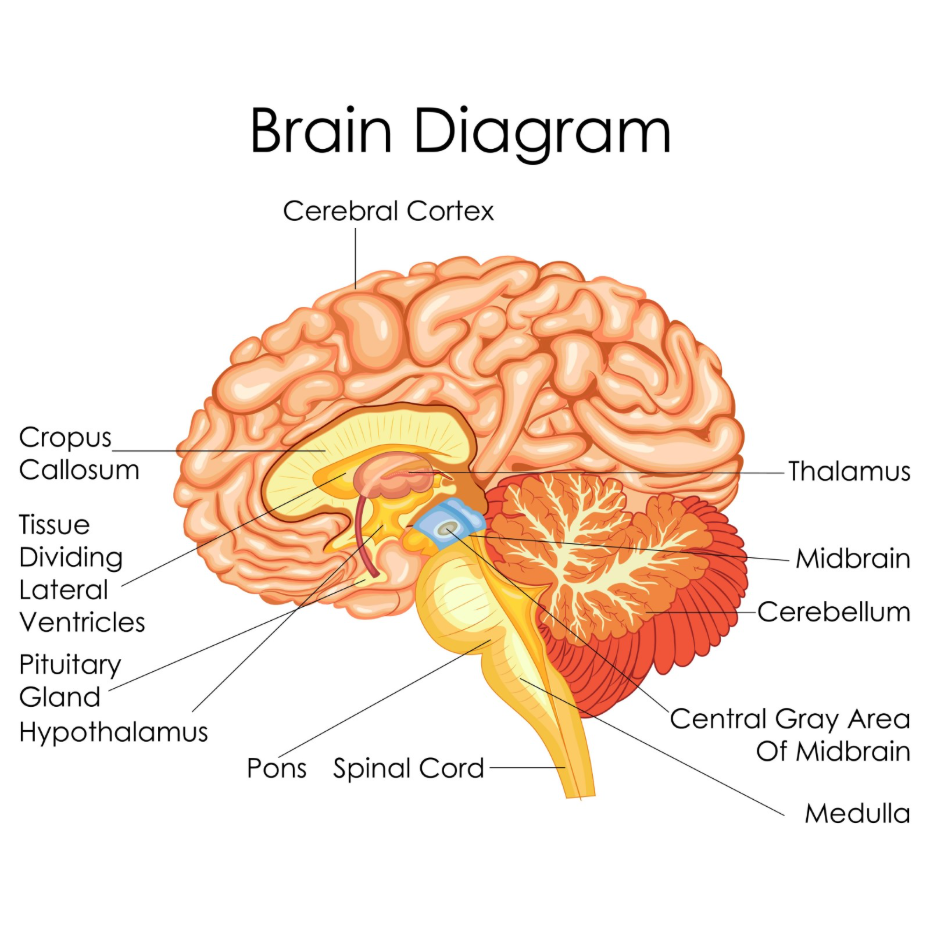
Gliomas begin when glial cells, which provide structural support and insulation for neurons, undergo abnormal genetic changes that lead to uncontrolled cell division. Unlike neurons, which transmit electrical signals, glial cells perform various maintenance tasks such as providing nutrients, maintaining the blood brain barrier, and producing myelin to speed up signal transmission. The NHS states that a brain tumour is a growth of cells in the brain that multiplies in an abnormal, uncontrollable way.
When these supportive cells become cancerous or form a mass, they are named according to the cell type they resemble. Because glial cells are found throughout the brain and spinal cord, gliomas can occur in many different locations. In the United Kingdom, pathologists examine tissue samples to see which specific glial line has become abnormal. Understanding the supportive nature of these cells helps explain why gliomas often grow by infiltrating the spaces between healthy neurons rather than forming a strictly self-contained lump. This invasive growth pattern is a key characteristic that UK clinical teams consider when planning management.
Primary Types of Glioma Tumours
There are several distinct types of gliomas, each named after the specific glial cell from which the tumour is thought to arise. The most common type is the astrocytoma, which develops from star-shaped cells called astrocytes that help regulate the brain’s environment. Oligodendrogliomas arise from cells that produce the protective fatty coating for nerve fibres, while ependymomas develop from cells lining the fluid-filled spaces of the brain. NICE clinical guidelines for brain tumours indicate that identifying the specific subtype of glioma is essential for determining the expected clinical behaviour and management plan.
| Glioma Subtype | Originating Cell | Common Characteristics |
| Astrocytoma | Astrocytes | Can range from slow-growing to highly aggressive. |
| Oligodendroglioma | Oligodendrocytes | Often slow-growing and may respond well to treatment. |
| Ependymoma | Ependymal cells | Frequently found near the fluid cavities or spinal cord. |
| Glioblastoma | Highly abnormal cells | The most aggressive form of Grade 4 astrocytoma. |
In the UK, specialists also look for specific molecular markers within these subtypes, such as the IDH mutation status. These genetic details provide more information about how the tumour is likely to respond to various therapies. By categorising gliomas in this way, the NHS ensures that patients receive a management strategy tailored to the specific biology of their tumour.
The WHO Grading System for Gliomas
In the United Kingdom, gliomas are graded from 1 to 4 using the World Health Organization (WHO) criteria to indicate how aggressive the tumour is and how quickly it is likely to progress. Grade 1 and 2 gliomas are considered low-grade, meaning the cells grow slowly and look relatively similar to healthy cells under a microscope. Grade 3 and 4 gliomas are high-grade or malignant, characterised by rapid cell division and a higher likelihood of invading healthy brain tissue.
A Grade 4 glioma, such as a glioblastoma, is the most aggressive type and requires urgent clinical intervention. Low-grade tumours may remain stable for long periods but are monitored closely because they have the potential to transform into higher-grade tumours over time. UK multidisciplinary teams use this grading system to decide on the frequency of follow-up scans and the timing of any active management. This standardised approach ensures that care is proportionate to the risk posed by the tumour’s growth rate. Accurate grading is achieved through a combination of high-resolution imaging and, where possible, a surgical biopsy to analyse the tissue directly.
Common Symptoms and Clinical Presentation
Symptoms of a glioma are determined by where the tumour is located in the brain and how much pressure it is putting on the surrounding neurological structures. Because gliomas often grow by infiltrating healthy tissue, they can disrupt various functions such as movement, speech, or sensory perception. General symptoms often result from increased intracranial pressure as the tumour occupies space within the rigid skull.
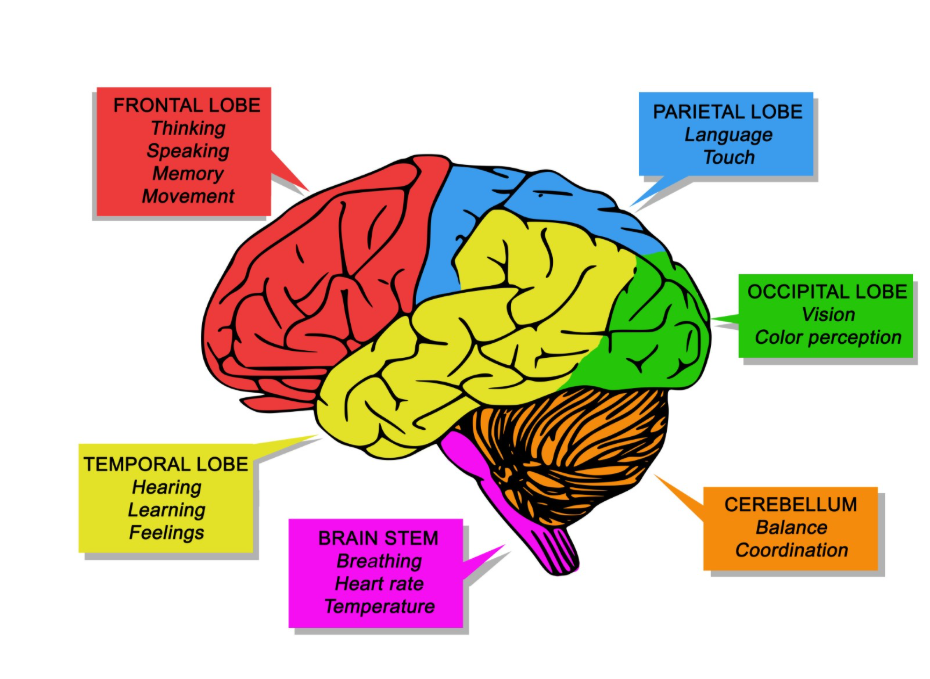
The GOV.UK health pages provide clinical profiles indicating that common symptoms of a brain tumour include new-onset headaches, seizures, and persistent changes in personality or vision. Headaches associated with gliomas are often worse in the morning and may be accompanied by nausea or vomiting. Focal symptoms depend on the lobe affected; for example, a glioma in the frontal lobe may cause weakness on one side of the body, while a temporal lobe tumour might affect memory or speech. In the UK, if these symptoms are persistent or follow a worsening pattern, they are treated as red flags that require urgent neurological investigation through a GP or hospital specialist.
The Diagnostic Process in the UK
The diagnostic pathway for a suspected glioma in the United Kingdom prioritises rapid access to advanced imaging followed by a specialist review to confirm the nature of the growth. If a patient presents with suspicious neurological signs, the first step is usually a CT or MRI scan to visualise the internal structures of the brain. An MRI scan with contrast dye is the preferred tool for identifying gliomas because it provides a detailed view of the tumour’s boundaries and its relationship with blood vessels.
The UK diagnostic pathway includes:
- Initial Imaging: Using MRI to identify the location and size of the mass.
- Specialist Referral: Assessment by a neurosurgeon or neurologist.
- Biopsy or Resection: Taking a tissue sample to confirm the grade and molecular type.
- MDT Review: A Multidisciplinary Team of experts discussing the results to plan management.
Following the imaging, a biopsy is often necessary because different types of gliomas can look similar on a scan but require different management approaches. In the UK, neurosurgeons aim to remove as much of the tumour as safely possible (resection) or take a small sample using a needle (needle biopsy). This tissue is then sent to a neuropathologist who performs the detailed cellular and genetic analysis required for a final diagnosis.
Management Pathways for Gliomas
Management of gliomas in the United Kingdom is highly integrated, involving a combination of surgery, radiotherapy, and systemic therapies depending on the grade and location of the tumour. For many low-grade gliomas, the clinical team may suggest a period of active surveillance, often called “watch and wait,” where the tumour is monitored with regular MRI scans. If a glioma is high-grade or causing significant symptoms, more active management is typically required to reduce the size of the mass and control its growth.
The UK approach focuses on:
- Surgical Resection: Removing the maximum amount of tumour while protecting brain function.
- Radiotherapy: Using targeted beams to destroy remaining abnormal cells.
- Systemic Therapy: Utilising medication to interfere with the tumour’s ability to divide.
- Supportive Care: Managing symptoms like seizures or swelling with appropriate medication.
Throughout the process, patients are supported by specialist nurses and allied health professionals who help manage the physical and emotional impact of the condition. In the UK, clinical trials are also an integrated part of the pathway, offering eligible patients access to emerging management options. The goal of every management plan is to achieve the best possible control of the glioma while ensuring the patient maintains their functional independence for as long as possible.
Conclusion
A glioma is a primary brain tumour originating from the supportive glial cells and is graded according to its growth rate and cellular characteristics. In the UK, the NHS follows a structured pathway of imaging, biopsy, and multidisciplinary review to determine the most effective management for each individual. While high-grade gliomas require urgent intervention, low-grade versions are often managed through careful monitoring and scheduled surgery. Understanding the specific type and grade of a glioma is essential for providing accurate information and clear expectations for the future. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is a glioma always cancerous?
In medical terms, Grade 3 and 4 gliomas are considered malignant (cancerous), while Grade 1 and 2 are low-grade, though they still require specialist monitoring.
Can a glioma spread to other parts of the body?
Primary gliomas rarely spread outside the brain or spinal cord, although they can spread to other areas within the central nervous system.
What causes a glioma to form?
The exact cause is usually unknown, but established risk factors in the UK include increasing age and previous exposure to high-dose radiation.
Can surgery cure a glioma?
For some low-grade gliomas, surgery can remove the entire mass, but because gliomas are often invasive, long-term monitoring is usually required.
How often will I need scans after a diagnosis?
In the UK, the frequency of MRI scans depends on the grade of the glioma and can range from every few months to once a year.
Are gliomas hereditary?
The vast majority of gliomas are sporadic and not passed through families, although a very small number are linked to rare genetic syndromes.
What is a glioblastoma?
A glioblastoma is the most common and aggressive form of high-grade glioma, categorised as a WHO Grade 4 astrocytoma.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding glioma brain tumours, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in surgery, emergency care, and clinical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
