Cerebral palsy is classified into several types based on the specific movement disorder present and the parts of the body affected. In the United Kingdom, the NHS uses these classifications to ensure that individuals receive the most appropriate therapy and support for their unique neurological needs. The condition is permanent but can be managed effectively through integrated clinical pathways.
What We’ll Discuss in This Article
- The four primary clinical classifications of cerebral palsy.
- How the location of brain injury determines the movement type.
- Functional differences between spastic, dyskinetic, and ataxic types.
- Geographical classifications including hemiplegia and diplegia.
- The role of mixed cerebral palsy in complex cases.
- Accessing specialist NHS multidisciplinary support for each type.
Spastic Cerebral Palsy
Spastic cerebral palsy is the most common type, characterised by increased muscle tone that leads to stiffness and difficulty with voluntary movements. This occurs when the injury is in the motor cortex or the pyramidal tracts of the brain, which are responsible for sending clear instructions to the muscles. The NHS states that spastic cerebral palsy means the muscles are stiff and tight, which makes it difficult to move and can reduce the range of movement in the joints.
In the United Kingdom, clinicians assess for spasticity by checking how a muscle responds to being stretched quickly. If the muscle reacts by tightening, it can lead to long-term issues such as contractures, where the muscles become permanently shortened. The management of this type often involves intensive physiotherapy to maintain flexibility and sometimes medications or surgery to reduce muscle tension. Because the stiffness can affect different parts of the body, the NHS further categorises spasticity based on which limbs are involved, ensuring that equipment and therapy are tailored to the individual’s specific mobility challenges.
Dyskinetic Cerebral Palsy
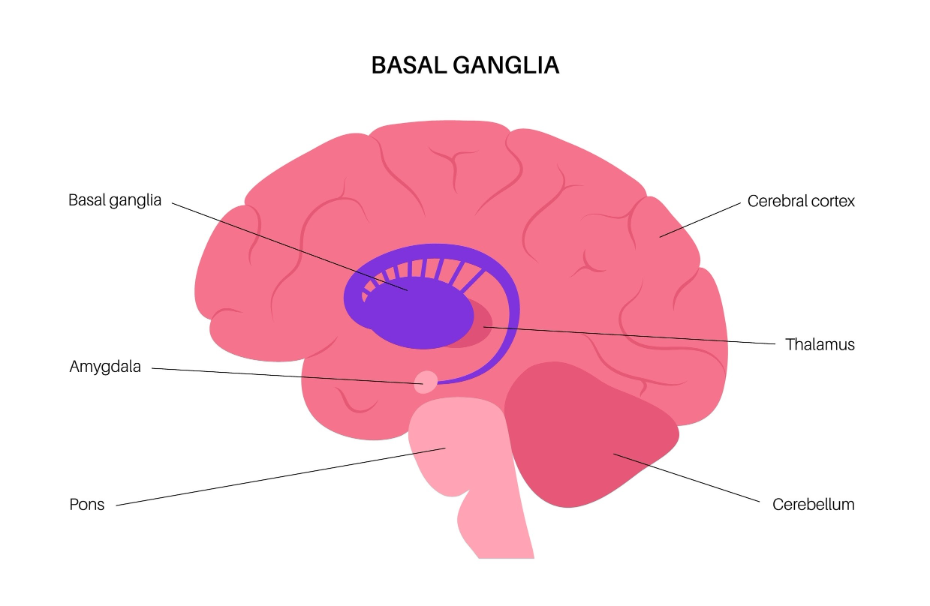
Dyskinetic cerebral palsy involves involuntary, uncontrolled movements that can be twisting, repetitive, or jerky, occurring when the injury is in the basal ganglia. The basal ganglia act as a filter for movement signals, and when they are damaged, “incorrect” signals reach the muscles, causing them to move without the person’s intent. NICE clinical guidelines for cerebral palsy indicate that dyskinetic movements often become more noticeable when the person is tired, excited, or attempting a purposeful task.
Individuals with this type may struggle to maintain a stable posture and might experience changes in muscle tone throughout the day, shifting from very stiff to very floppy. This type is often further divided into athetoid (slow, writhing movements) and dystonic (twisting and repetitive movements). In the UK, speech and language therapists are frequently involved in the care of people with dyskinetic cerebral palsy, as the condition can affect the muscles used for talking and swallowing. Integrated support focuses on providing postural stability and using communication aids where necessary to support functional independence.
Ataxic Cerebral Palsy
Ataxic cerebral palsy is a less common type that primarily affects balance and depth perception, resulting from an injury to the cerebellum. The cerebellum is the part of the brain responsible for coordinating fine motor skills and ensuring that movements are smooth and precise.
| Movement Feature | Characteristics of Ataxia | Impact on Daily Life |
| Balance | Unsteady or shaky gait. | Increased risk of falls; wide walking stance. |
| Precision | Difficulty with fine motor tasks. | Challenges with writing or fastening buttons. |
| Coordination | Overreaching or underreaching. | Difficulty with hand-eye coordination tasks. |
| Intention Tremor | Shaking that worsens during a task. | Spilling drinks or difficulty using cutlery. |
In the United Kingdom, ataxic cerebral palsy is often identified when a child begins to reach for toys or starts to walk with a wide, unsteady gait. Unlike spasticity, muscle tone in ataxic cases is often normal or slightly low (hypotonia). Management focuses on balance exercises and occupational therapy to develop compensatory strategies for fine motor tasks. The NHS provides a safety net of support to help individuals navigate these coordination challenges, often using specialist equipment to improve stability during daily activities.
Geographical Classifications of Movement
Beyond the type of movement disorder, cerebral palsy is also classified geographically by the parts of the body that are impacted by the brain injury. In the United Kingdom, these terms help the multidisciplinary team understand the extent of the motor impairment and plan for appropriate home and school adaptations.
Common geographical terms used by the NHS include:
- Hemiplegia: Only one side of the body is affected, usually due to an injury on the opposite side of the brain.
- Diplegia: Both legs are primarily affected, with the arms being less impacted or not affected at all.
- Quadriplegia: All four limbs and the trunk are affected, often involving challenges with neck and head control.
- Monoplegia: A very rare form where only one limb is affected.
The GOV.UK health pages provide clinical profiles indicating that understanding the geographical distribution of motor impairment is essential for coordinating long-term social and health support. For example, a child with hemiplegia may focus on bimanual therapy to encourage the use of both hands, while someone with diplegia may prioritise walking aids. This classification system ensures that the goals of the therapy team are aligned with the physical reality of the individual’s condition, providing a clear framework for progress.
Mixed Cerebral Palsy
Mixed cerebral palsy occurs when an individual shows symptoms of more than one type of the condition, usually because the brain injury has impacted multiple regions of the motor control system. It is common for a person to have a combination of spastic and dyskinetic features, requiring a more complex and multifaceted management plan.
The challenges of mixed cerebral palsy in the UK include:
- Variable Muscle Tone: Managing both stiffness and involuntary movements simultaneously.
- Complex Therapy Needs: Requiring a wider range of specialist interventions from various therapists.
- Medication Coordination: Carefully balancing different drugs to manage conflicting movement symptoms.
- Postural Management: Using highly specialised seating and equipment to support a stable body position.
In the United Kingdom, patients with mixed cerebral palsy are monitored closely by paediatric neurologists to ensure their management plan remains effective as they grow. The integrated care pathway ensures that the various specialists involved such as physiotherapists and occupational therapists work together to address the diverse symptoms. This collaborative approach is vital for ensuring that the individual can achieve their functional potential despite the complexity of their neurological profile.
Accessing Integrated NHS Support for All Types
The United Kingdom provides a comprehensive framework of integrated support for individuals with all types of cerebral palsy, ensuring that their medical, social, and educational needs are met through a single, coordinated pathway. This support is tailored to the specific type and severity of the condition identified during the diagnostic process.
The UK support framework involves:
- Child Development Centres: Hubs where various therapists and doctors provide coordinated care.
- Specialist Nurses: Acting as a consistent point of contact for families to navigate the system.
- Education, Health and Care (EHC) Plans: Legal documents ensuring the right support is available in school.
- Transition Services: Helping young people move from paediatric to adult healthcare teams.
By utilising this integrated framework, the NHS ensures that the management of cerebral palsy is consistent and evidence based. Accessing these services through a GP or hospital consultant ensures that the care is medically supervised and aligned with national quality standards. This professional safety net provides individuals and their families with the reassurance that they have access to the full range of expertise required to manage the lifelong impact of the condition effectively.
Conclusion
Cerebral palsy exists in several distinct types, including spastic, dyskinetic, and ataxic, each defined by the nature of the movement disorder and the brain region affected. In the UK, the NHS uses these classifications alongside geographical markers like hemiplegia to provide tailored, multidisciplinary support. While some individuals have a single type, many experience mixed symptoms that require a more complex management plan. Following a structured clinical pathway with the multidisciplinary team ensures the best possible functional outcomes for every individual. The UK healthcare system provides a life-long safety net for managing these neurological challenges. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is it possible for the type of cerebral palsy to change over time?
The underlying brain injury is static, but as a child grows, their movement patterns may become clearer, leading to a more refined classification.
Can a person have more than one type of cerebral palsy?
Yes; this is known as mixed cerebral palsy and occurs when multiple areas of the brain’s motor control system are affected.
Why is spastic cerebral palsy the most common type?
The motor cortex and its pathways are large areas of the brain, making them more statistically likely to be involved in a developmental injury.
How does a doctor decide which type my child has?
UK specialists use physical examinations to check muscle tone, reflexes, and coordination, alongside history and brain imaging.
Does the type of cerebral palsy affect intelligence?
The type of movement disorder does not determine intelligence, although some people may have associated learning needs depending on the extent of the injury.
Which type is the most difficult to manage?
Every individual is different; difficulty is often more related to the severity of the symptoms rather than the specific type itself.
Can adults be re-classified if their movements change?
While the diagnosis remains the same, an adult’s functional needs are reviewed by the NHS to ensure their support remains appropriate.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the types of cerebral palsy, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in general surgery, cardiology, and emergency medicine. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
