A brain tumour can develop in almost any part of the central nervous system, including the main sections of the brain, the protective membranes, or the cranial nerves. Because the brain is the control centre for the entire body, the specific location of a growth determines which physical or cognitive functions may be affected. In the United Kingdom, healthcare professionals categorise brain tumours by their anatomical location to help predict their behaviour and guide the management process. The UK healthcare system utilise a structured approach to identify these locations using advanced imaging, ensuring that care is aligned with national clinical standards. Understanding the different areas where a tumour can form is essential for recognising how symptoms manifest. By following evidence-based protocols established by the NHS and NICE, clinicians aim to provide targeted care that addresses the specific challenges posed by the tumour’s position within the skull.
What We’ll Discuss in This Article
- Tumours occurring in the cerebrum and its four distinct lobes.
- The impact of growths within the cerebellum and the brainstem.
- How tumours develop in the meninges and the pituitary gland.
- The clinical significance of tumours affecting the cranial nerves.
- How location influences the diagnostic and management pathway in the UK.
- The relationship between anatomical position and neurological symptoms.
Tumours in the Cerebrum and Its Four Lobes
The cerebrum is the largest part of the brain and is frequently the site where primary brain tumours develop, with symptoms varying depending on which of its four lobes is affected. The cerebrum is divided into the frontal, parietal, temporal, and occipital lobes, each responsible for specific tasks such as personality, movement, and sensory processing. The NHS states that a brain tumour is a growth of cells in the brain that multiplies in an abnormal, uncontrollable way, and its symptoms depend on the part of the brain affected.
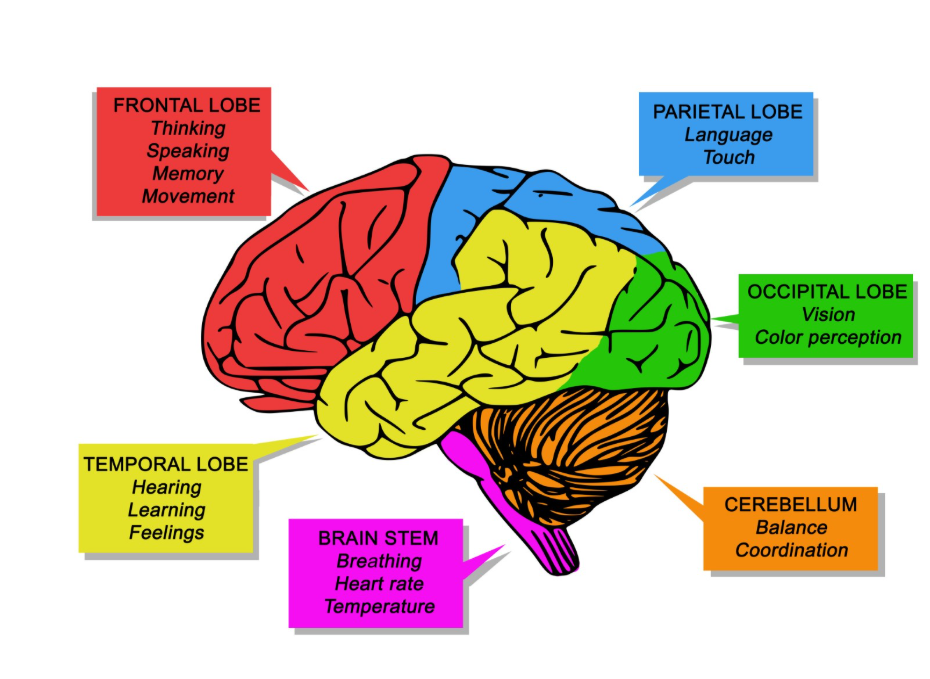
If a tumour grows in the frontal lobe, it may lead to changes in personality or weakness on one side of the body. A growth in the temporal lobe might affect speech or memory, while a parietal lobe tumour can interfere with the ability to recognise objects or understand spatial relationships. Occipital lobe tumours are primarily associated with vision changes. In the United Kingdom, clinicians use detailed neurological examinations to identify which lobe may be compromised before confirming the location with an MRI scan. Because the cerebrum occupies the most space within the skull, it is the most common area for both primary and secondary tumours to be identified.
The Cerebellum and the Brainstem
Tumours can also develop in the cerebellum and the brainstem, which are located at the base of the brain and control essential functions such as balance, coordination, and breathing. The cerebellum, often called the small brain, sits at the back of the skull and is a common site for certain childhood brain tumours. NICE clinical guidelines for brain tumours indicate that the location of a tumour in the posterior fossa, which includes the cerebellum and brainstem, requires specific management strategies due to the density of vital structures.
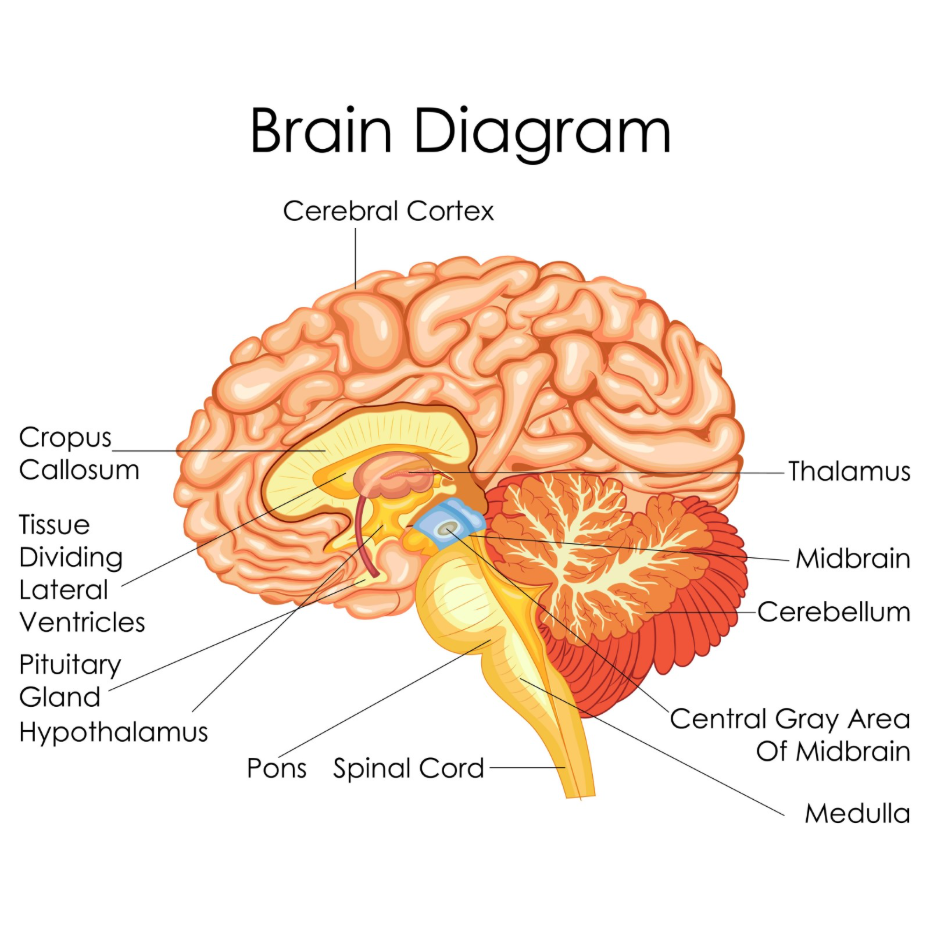
A tumour in the cerebellum typically causes issues with coordination, leading to a staggered walk or difficulty with fine motor skills. The brainstem is even more critical, as it connects the brain to the spinal cord and regulates automatic functions like heart rate and blood pressure. Because the brainstem is a very compact area, even a small tumour can have significant clinical implications. In the UK, tumours in these locations are managed with extreme care, as surgical access is often more complex than in the cerebrum. Clinicians prioritise the preservation of these life-sustaining pathways during any management intervention.
Meningiomas and the Protective Membranes
Not all brain tumours grow within the brain tissue itself; many develop in the meninges, which are the three layers of protective membranes that surround the brain and spinal cord. These tumours, known as meningiomas, are the most common primary brain tumour in adults in the United Kingdom.
Most meningiomas are non-cancerous and grow slowly, often pushing on the surface of the brain rather than invading it.
| Brain Area | Common Tumour Type | Primary Functions Affected |
| Cerebrum | Glioma | Thought, movement, speech, vision. |
| Meninges | Meningioma | Varies based on the area of pressure. |
| Cerebellum | Medulloblastoma | Balance, coordination, motor skills. |
| Brainstem | Glioma | Heart rate, breathing, swallowing. |
Because these tumours grow on the outside of the brain, they can sometimes reach a significant size before they cause symptoms. In the UK, many are found incidentally when a patient has a scan for an unrelated reason. If they do cause symptoms, it is usually because they are pressing on a specific part of the cerebrum or increasing the overall pressure within the skull.
The Pituitary Gland and Cranial Nerves
Tumours can develop in the pituitary gland or along the cranial nerves, affecting the body’s hormonal balance or specific senses such as hearing and balance. The pituitary gland is a pea-sized structure at the base of the brain that produces hormones regulating growth, metabolism, and reproduction. A tumour here can cause hormonal imbalances or press on the optic nerves, leading to vision loss.

Cranial nerve tumours, such as acoustic neuromas, grow on the nerves that transmit sound and balance information from the inner ear to the brain. These typically cause hearing loss in one ear or dizziness. The GOV.UK health pages provide clinical profiles for various intracranial tumours, including those affecting the pituitary and cranial nerves, to guide specialist care across the NHS. In the United Kingdom, these are often managed by a multidisciplinary team that includes neurosurgeons and endocrinologists to ensure that both the physical growth and any hormonal changes are addressed.
Location and the UK Management Pathway
The specific part of the brain where a tumour is found dictates the complexity of the management pathway and the types of specialists involved in the UK clinical team. Once a tumour’s location is identified on a scan, a Multidisciplinary Team (MDT) meets to discuss the findings.
The UK management pathway considers:
- Surgical Accessibility: Whether the tumour can be reached safely without damaging eloquent (vital) areas.
- Functional Impact: Which neurological symptoms are currently present and how they might be managed.
- Grading and Type: Identifying the cellular makeup through a biopsy or surgery.
- Radiotherapy Planning: Determining if targeted radiation is needed for tumours in sensitive locations like the brainstem.
Because the brain is a highly mapped organ, UK specialists can often predict exactly which challenges a patient will face based on the tumour’s coordinates. This integrated approach ensures that the management plan is as precise as possible, aiming to remove or control the growth while minimising the risk of permanent neurological deficit. Long-term care often includes rehabilitation to support any functions that were affected by the tumour’s location.
Conclusion
Brain tumours can develop in various parts of the brain, including the lobes of the cerebrum, the cerebellum, the brainstem, and the protective meninges. The location of the growth is a primary factor in determining the symptoms a person experiences and the management strategy used in the UK. While some areas are more accessible for surgery, others require highly specialised care to protect vital functions like breathing and balance. Consistent clinical monitoring and accurate imaging are essential for managing tumours regardless of their position. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can a tumour be in two parts of the brain at once?
Yes, some tumours can grow large enough to cross into adjacent lobes or spread through the cerebrospinal fluid to multiple locations.
Is a tumour in the frontal lobe more dangerous than one in the temporal lobe?
Danger depends on the grade and size; however, different locations cause different symptoms, such as personality changes versus speech issues.
Are tumours in the brainstem always cancerous?
Not necessarily, but any growth in the brainstem is treated with great urgency because there is no extra room for swelling in that area.
Can a brain tumour affect my sense of smell?
Yes, a tumour located at the base of the frontal lobes near the olfactory nerves can interfere with the ability to smell.
How do doctors see exactly where the tumour is?
The NHS uses high-resolution MRI scans which provide detailed cross-sectional images of the brain from multiple angles.
Does the location tell the doctor if it is benign or malignant?
No; while certain types are more common in specific areas, only a biopsy or laboratory analysis can definitively tell the grade of the cells.
Can a tumour grow on the spinal cord as well?
Yes, the same types of tumours that affect the brain can also develop in the spinal cord, as they are both part of the central nervous system.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the locations of brain tumours, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in emergency care, neurosurgery wards, and clinical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
