The fundamental difference between Irritable Bowel Syndrome, or IBS, and Inflammatory Bowel Disease, or IBD, lies in the nature of the condition: IBS is a functional disorder, whereas IBD is a structural, inflammatory disease. IBS affects how the gut works and moves, causing symptoms like bloating and abdominal pain without causing visible damage to the digestive tract. In contrast, IBD involves chronic inflammation, ulcers, and physical damage to the bowel wall, which can be seen during clinical investigations. While they share overlapping symptoms like abdominal cramping and altered bowel habits, IBD is a serious autoimmune condition that requires distinct medical management to prevent long term complications.
What We Will Cover in This Article
- Distinguishing between functional disorders and inflammatory diseases
- The primary symptoms of IBS versus the clinical markers of IBD
- How clinical investigations like colonoscopies differentiate the two
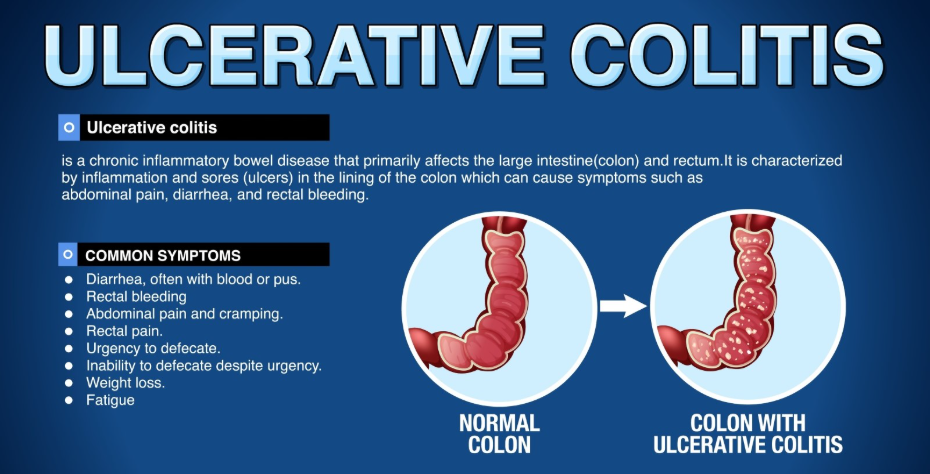
- Understanding the types of IBD: Crohn disease and Ulcerative Colitis
- Why IBS does not increase the risk of bowel cancer or surgery
- Clinical red flags that suggest IBD rather than IBS
- Standard UK diagnostic pathways for chronic digestive issues
IBS vs IBD: A Comparison of Core Features
IBS is often described as a brain-gut disorder where the nerves in the digestive system become hypersensitive. This leads to irregular muscle contractions, but the gut remains structurally healthy. IBD, however, is an umbrella term for conditions like Crohn disease and Ulcerative Colitis, where the body’s immune system attacks the bowel. This results in visible inflammation, bleeding, and narrowing of the intestines. Unlike IBS, which is managed primarily through diet and lifestyle, IBD often requires powerful immunosuppressant medications or surgery to manage the physical damage to the gut.
Identifying the Primary Causes
The origins of these two conditions involve different biological pathways.
Causes of IBS
The exact cause of IBS is unknown, but it is often triggered by:
- Gut Sensitivity: Increased sensitivity to the stretching of the gut wall.
- Motility Issues: Food moving too quickly or too slowly through the digestive tract.
- Stress and Mental Health: The strong connection between the nervous system and the gut.
- Post-Infectious IBS: Symptoms that begin after a severe bout of food poisoning or gastroenteritis.
Causes of IBD
IBD is an autoimmune condition where the immune system malfunctions. Triggers include:
- Genetics: A family history of IBD increases individual risk.
- Immune System Response: An overactive immune response to bacteria or viruses in the gut.
- Environmental Factors: Factors such as smoking or specific dietary patterns that may trigger inflammation in genetically predisposed individuals.
Key Symptom Differences
Although both cause abdominal pain and changes in bowel habits, certain symptoms are exclusive to IBD.
| Feature | Irritable Bowel Syndrome (IBS) | Inflammatory Bowel Disease (IBD) |
| Inflammation | No visible inflammation | Chronic, visible inflammation |
| Blood in Stool | Very rare (unless from piles) | Common symptom |
| Weight Loss | Unintentional weight loss is rare | Significant unintentional weight loss |
| Night Symptoms | Rarely wakes the patient from sleep | Frequently wakes the patient |
| Fever | Not a symptom of IBS | Common during flare-ups |
| Bowel Damage | No permanent damage to the gut | Can cause scarring, ulcers, and fistulas |
The Diagnostic Pathway in the UK
Clinicians follow a specific protocol to ensure an accurate diagnosis, as treating IBD as IBS can be dangerous.
In the UK, a GP will typically start with blood tests to look for markers of inflammation, such as C-Reactive Protein, or CRP. A specific stool test called a Faecal Calprotectin test is highly effective at distinguishing the two; a high level strongly suggests IBD, while a normal level points toward IBS. If IBD is suspected, the patient is referred for an endoscopy or colonoscopy, where a camera is used to look for physical signs of disease and take biopsies of the gut lining.
To Summarise
The difference between IBS and IBD is the presence of physical damage and inflammation. IBS is a functional issue that is uncomfortable but does not cause permanent harm to the body. IBD is a chronic inflammatory disease that requires specialist medical intervention to prevent serious complications. Understanding these differences is essential for ensuring that patients receive the correct clinical support and treatment plan.
If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can IBS turn into IBD over time?
No. They are two separate conditions with different causes. However, it is possible for a person to have both conditions simultaneously.
Does IBS increase the risk of bowel cancer?
No. IBS does not cause inflammation or changes to the cells of the bowel, so it does not increase cancer risk. Chronic IBD, however, does require regular screening for cancer.
Why does my IBS feel as painful as IBD?
Pain levels are not a good indicator of the severity of the condition. Nerve hypersensitivity in IBS can cause intense pain even though there is no physical damage.
Is there a cure for either condition?
There is currently no cure for either, but both are highly manageable. IBS is managed with diet and stress reduction, while IBD is managed with medication and occasionally surgery.
Can stress cause IBD?
Stress does not cause IBD, but it can certainly trigger a flare-up of symptoms in someone who already has the condition.
What is the Faecal Calprotectin test?.
It is a simple stool test that measures a protein released by inflamed gut cells. It is the most common way UK doctors rule out IBD.
Are the diets for IBS and IBD the same?
No. Many people with IBS follow the Low FODMAP diet. People with IBD may need specific low-residue diets during flare-ups but generally follow different nutritional guidelines.
Authority Snapshot
This article was reviewed by Dr. Rebecca Fernandez, a UK-trained physician with an MBBS and extensive experience across general surgery, internal medicine, and emergency care. Dr. Fernandez has managed complex gastrointestinal cases in both inpatient and outpatient settings. She specialises in evidence-based treatment planning and the integration of mental well-being strategies for patients managing chronic functional and inflammatory disorders.
