Chronic pancreatitis is a progressive inflammatory condition that can significantly impact the endocrine function of the pancreas, leading to the development of diabetes and complex blood sugar fluctuations. Healthcare professionals in the UK utilise structured monitoring and diagnostic pathways to identify early signs of endocrine failure in patients with known pancreatic damage. By following established clinical frameworks from the NHS and the National Institute for Health and Care Excellence, medical teams can provide targeted insulin therapy and nutritional support. Understanding the biological link between permanent pancreatic scarring and metabolic health allows patients to engage in proactive management to reduce the risk of long-term complications.
What We’ll Discuss in This Article
- The biological role of the pancreas in blood sugar regulation
- How permanent scarring destroys insulin producing cells
- Defining Type 3c diabetes and how it differs from other types
- Common symptoms of blood sugar problems in pancreatic patients
- UK clinical protocols for monitoring glucose levels in chronic cases
- Management strategies for stabilising blood sugar and nutrition
- The importance of lifestyle changes to prevent further organ damage
Chronic pancreatitis leads to diabetes because the progressive inflammation causes permanent scarring that destroys the islet cells responsible for producing insulin and glucagon
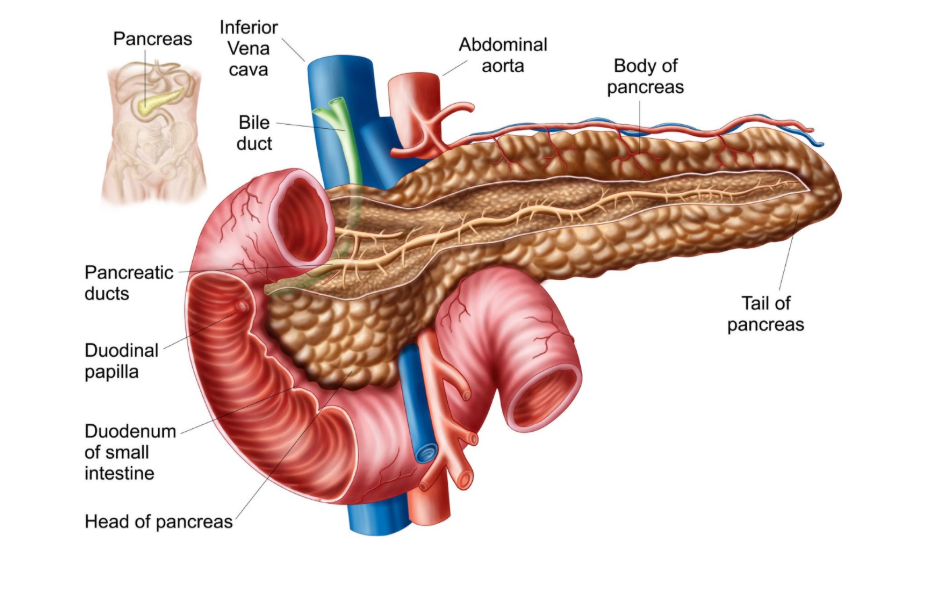
The pancreas contains clusters of cells known as the Islets of Langerhans, which secrete hormones directly into the bloodstream to regulate glucose. Chronic pancreatitis is where the pancreas has been permanently damaged from inflammation over many years, which can lead to diabetes if the insulin producing cells are destroyed. As the inflammatory process continues, healthy pancreatic tissue is replaced by non functional scar tissue. This loss of cellular mass means the organ can no longer produce sufficient insulin to lower blood sugar or enough glucagon to raise it when it falls too low. In the United Kingdom, this metabolic shift is a well documented complication of long term pancreatic disease, requiring lifelong clinical management to maintain health.
Understanding the characteristics of Type 3c diabetes
Diabetes resulting from chronic pancreatitis is distinct from Type 1 or Type 2 diabetes and is medically classified as Type 3c diabetes. Unlike Type 2 diabetes, which is often characterised by insulin resistance, Type 3c is caused by a physical lack of hormone producing cells. Furthermore, because the pancreas also loses the ability to produce glucagon, patients are at a higher risk of experiencing sudden drops in blood sugar, known as hypoglycaemia. Acute pancreatitis is where the pancreas becomes inflamed over a short period of time, but repeated episodes can lead to the permanent damage of chronic pancreatitis and subsequent diabetes. Within the NHS, this form of diabetes is often managed by specialist teams who understand the “brittle” nature of blood sugar levels when both primary regulatory hormones are missing.
Symptoms of blood sugar problems in pancreatic patients
Patients with chronic pancreatitis should be vigilant for symptoms that indicate the onset of diabetes or poorly regulated blood sugar. Common signs include increased thirst, frequent urination, particularly at night, and persistent fatigue or blurred vision. Because the pancreas is also failing to produce digestive enzymes, these symptoms may occur alongside unintended weight loss and oily stools.
According to the National Institute for Health and Care Excellence, people with chronic pancreatitis should be offered at least annual monitoring for diabetes using blood tests. Recognising these changes early is vital, as high blood sugar levels can damage blood vessels and nerves over time, while low blood sugar can cause immediate dizziness, confusion, or fainting.
Clinical monitoring and diagnosis in the UK
In the United Kingdom, the diagnostic process for pancreatic related diabetes involves regular screening of blood glucose markers. The most common test is the HbA1c test, which measures the average blood sugar levels over the previous two to three months. Because chronic pancreatitis is a progressive condition, a patient may have normal blood sugar for several years before the damage reaches a threshold where diabetes develops. UK clinicians also assess the patient’s nutritional status, as malabsorption of nutrients can complicate the management of blood sugar. Annual reviews are a standard part of NHS care for chronic pancreatitis patients, ensuring that any transition to an endocrine deficient state is identified and treated promptly.
Comparison of Diabetes Types
| Feature | Type 1 Diabetes | Type 2 Diabetes | Type 3c (Pancreatic) |
| Primary Cause | Autoimmune destruction | Insulin resistance | Physical organ damage/scarring |
| Hormones Lost | Primarily Insulin | None (Ineffective use) | Insulin and Glucagon |
| Weight Link | Often lean at onset | Often linked to obesity | Often linked to weight loss |
| Management | Insulin injections | Diet, tablets, or insulin | Insulin and enzyme replacement |
| Sugar Stability | Variable | Usually more stable | “Brittle” (High risk of lows) |
Treatment and management of pancreatic diabetes
The management of Type 3c diabetes in the UK focuses on replacing the missing hormones while supporting the patient’s digestive needs. Most patients eventually require insulin therapy to regulate their blood sugar levels. However, because these patients also lack digestive enzymes, they must take Pancreatic Enzyme Replacement Therapy (PERT) with their meals to ensure food is absorbed. Without proper digestion, insulin doses cannot be accurately timed with the absorption of glucose, leading to dangerous blood sugar swings. NHS specialists, including diabetologists and dietitians, work together to create a balanced plan that addresses both the endocrine and exocrine failures of the scarred pancreas.
Prevention and lifestyle considerations
While the scarring of chronic pancreatitis is irreversible, certain lifestyle modifications can help preserve remaining organ function and make blood sugar easier to manage. The complete avoidance of alcohol and smoking is the most critical recommendation in the UK, as both significantly accelerate the rate of pancreatic fibrosis and increase the risk of pancreatic cancer. Maintaining a healthy, balanced diet with the support of a dietitian helps to stabilise glucose levels and prevents the malnutrition that often accompanies pancreatic disease. By protecting the remaining healthy tissue, individuals can slow the progression of endocrine failure and reduce the severity of the blood sugar problems associated with chronic pancreatic damage.
Conclusion
Chronic pancreatitis frequently leads to Type 3c diabetes because permanent scarring destroys the cells that produce insulin and glucagon. This form of diabetes is often more complex to manage due to the simultaneous loss of digestive enzymes and a higher risk of low blood sugar. In the UK, annual screening and specialist multidisciplinary care are essential for managing these metabolic changes. Adhering to lifestyle advice regarding alcohol and smoking is vital for preserving remaining organ function. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why is it called Type 3c diabetes?
It is a specific classification used for diabetes that is caused by diseases of the exocrine pancreas, such as chronic pancreatitis or cystic fibrosis.
Can I prevent diabetes if I already have chronic pancreatitis?
Stopping smoking and drinking alcohol can slow the rate of scarring, which may delay or prevent the onset of diabetes in some cases.
Is pancreatic diabetes harder to manage than Type 2?
It can be, as the loss of glucagon makes you more prone to low blood sugar, and malabsorption makes it harder to time insulin with meals.
Will I always need insulin if I develop this?
Most people with Type 3c diabetes eventually require insulin because the organ is physically unable to produce enough of the hormone.
Does a high-sugar diet cause pancreatic diabetes?
No, this form of diabetes is caused by physical damage to the organ tissue rather than dietary sugar intake, although diet is important for management.
Can children get Type 3c diabetes?
Yes, if a child has chronic pancreatitis due to genetic factors or trauma, they can develop pancreatic diabetes as they grow.
How often should my blood sugar be checked?
NHS guidelines typically recommend at least an annual HbA1c blood test for anyone with a diagnosis of chronic pancreatitis.
Authority Snapshot (E-E-A-T Block)
This article was developed by the Medical Content Team to provide clear education on the metabolic consequences of pancreatic disease. The content has been reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine and intensive care, to ensure absolute alignment with NHS and NICE clinical guidance. Our purpose is to help the public understand the link between organ damage and diabetes through factual reporting.
