A Computed Tomography (CT) scan is a highly effective tool for identifying many structural abnormalities in the head, yet it cannot detect every type of brain tumour, particularly those that are small or slow growing. While a CT scan is often the first investigation performed in an emergency clinical setting, it lacks the fine detail required to visualise certain low-grade or deep-seated growths that are better identified through Magnetic Resonance Imaging (MRI). In the United Kingdom, healthcare professionals use CT scans as a rapid triage tool to rule out immediate life-threatening conditions before proceeding to more detailed neuroimaging if a tumour is still suspected. Understanding the specific strengths and limitations of CT technology is essential for patients as they navigate the diagnostic pathways provided by the NHS. By following evidence-based protocols established by NICE, medical teams ensure that the choice of scan is appropriate for the patient’s symptoms and the suspected nature of the neurological condition.
What We’ll Discuss in This Article
- The role of CT scans as an initial triage tool in UK emergency care.
- Technical limitations of CT in identifying small or low-grade tumours.
- Why certain brain regions are more difficult to visualise with X-ray technology.
- The importance of contrast agents in improving CT detection rates.
- A comparison between CT and MRI for definitive tumour diagnosis.
- The UK clinical pathway for follow-up imaging when a CT is inconclusive.
The Role of CT scans in Emergency Triage
CT scans are used as a primary diagnostic tool in the United Kingdom when a patient presents with acute neurological symptoms because they are fast, accessible, and highly reliable for detecting large masses or bleeding. A CT scan uses a series of X-rays to create cross-sectional images of the brain, allowing doctors to quickly identify structural shifts or signs of increased intracranial pressure. The NHS states that a CT scan may be used to help diagnose a brain tumour or to check for other problems, such as a brain haemorrhage.
Because the scan takes only a few minutes, it is ideal for patients who are seriously ill or who cannot remain still for the longer duration required by an MRI. In the UK, if a CT scan shows a significant abnormality, the patient is often fast-tracked to a neurosurgical unit for further assessment. However, clinicians recognize that a “normal” CT result does not always rule out a brain tumour entirely, especially if the patient’s symptoms are persistent or suggest a very small growth. The speed of CT makes it an essential component of the emergency diagnostic framework, but it is frequently viewed as a preliminary step rather than a final definitive test.
Technical Limitations in Detecting Certain Tumours
A CT scan may fail to detect every brain tumour because it relies on differences in tissue density, and some slow-growing or low-grade tumours can have a density very similar to healthy brain tissue. These tumours, such as certain types of low-grade gliomas, may not show up clearly on a CT scan because they do not cause significant swelling or contain calcium, which would otherwise make them visible to X-ray technology. NICE clinical guidelines for brain tumours indicate that if a CT scan is negative but clinical suspicion of a tumour remains high, an MRI should be performed as the next diagnostic step.
Furthermore, CT scans are less effective at identifying very small tumours, particularly those that are only a few millimetres in size. The resolution of a CT scan is generally lower than that of an MRI when it comes to soft-tissue differentiation. This means that while a CT is excellent for seeing bone and blood, it may miss subtle changes in the brain’s “white matter” where some tumours originate. In the UK healthcare system, radiologists are trained to look for indirect signs of a tumour, such as a slight shift in the brain’s midline, even if the tumour itself is not clearly visible. If these subtle signs are present, further detailed imaging is mandatory to ensure an accurate diagnosis.
Difficult Brain Regions and Bone Interference
Some areas of the brain are more challenging to visualise with a CT scan because of interference from the surrounding thick bones of the skull, which can obscure small tumours. The “posterior fossa,” the area at the back of the head containing the cerebellum and brainstem, is a common site for tumours where CT scans are known to have limitations. The dense bone at the base of the skull can create “artefacts” or shadows on the CT image, making it difficult to see small growths in these vital areas.
| Scan Feature | Computed Tomography (CT) | Magnetic Resonance Imaging (MRI) |
| Primary Technology | Ionising Radiation (X-rays) | Strong Magnetic Fields |
| Detection of Bone | Excellent; very detailed | Low; bone appears dark |
| Soft Tissue Detail | Moderate; less sensitive | High; detects subtle changes |
| Posterior Fossa View | Can be obscured by bone | Excellent; very clear |
| Scan Duration | 5 to 10 minutes | 30 to 60 minutes |
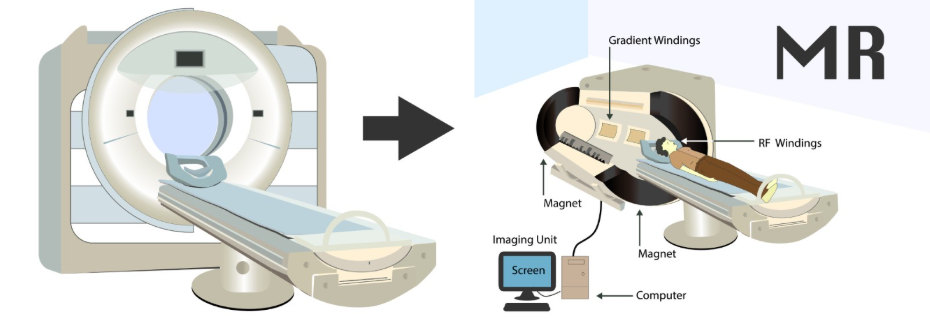
Because an MRI does not use X-rays, it is not affected by bone density in the same way, allowing for a clear view of the entire brain including the base and the spinal cord junction. In the United Kingdom, if a patient presents with symptoms such as unsteadiness or double vision which may suggest a tumour in the posterior fossa specialists will often prioritise an MRI. This ensures that the dense bone of the skull does not hide a tumour that would be easily missed on a standard CT. Understanding these regional difficulties is a key part of the diagnostic decision-making process for UK neurological teams.
The Use of Contrast Agents to Improve Detection
Contrast agents are frequently used during CT scans in the United Kingdom to improve the visibility of brain tumours by highlighting areas where the blood-brain barrier has been disrupted. This agent, usually containing iodine, is injected into a vein in the arm before the scan to make certain tissues appear brighter on the X-ray images. The GOV.UK health pages provide clinical profiles indicating that contrast-enhanced imaging is a standard requirement for assessing the vascularity and potential grade of a suspected brain tumour.
Many malignant or high-grade tumours have a high blood supply and “take up” the contrast, making them much easier for the radiologist to detect on a CT scan. However, many low-grade tumours do not absorb contrast in the same way, which is another reason why they may remain invisible on a CT even with the use of dye. In the UK, clinicians screen patients for kidney function and allergies before administering contrast to ensure the procedure is safe. While contrast significantly improves the detection rate of many tumours, it does not overcome all the inherent limitations of CT technology, meaning an MRI may still be required if the clinical picture remains unclear.
Comparison with MRI for Definitive Diagnosis
While CT is an excellent tool for rapid screening, MRI is considered the gold standard for the definitive diagnosis of a brain tumour in the UK because of its superior ability to differentiate between various types of soft tissue. An MRI uses powerful magnets and radio waves to create detailed multi-dimensional images that show the exact boundaries of a tumour and its relationship with healthy brain structures. This level of detail is necessary for neurosurgeons to plan a biopsy or surgical removal safely.

The superiority of MRI in tumour detection lies in its sensitivity to water and chemical changes within the brain. Small tumours that do not alter the density of the brain enough for a CT scan to detect will often show up clearly on an MRI as areas of “abnormal signal.” In the United Kingdom, almost every patient who has a tumour identified on a CT scan will subsequently undergo an MRI to provide the multidisciplinary team with the most accurate biological information. MRI is the preferred tool for identifying gliomas, meningiomas, and pituitary tumours, ensuring that the management plan is based on the highest quality data available within the NHS.
UK Clinical Pathways for Follow-up Imaging
The United Kingdom has established integrated care pathways to ensure that patients whose symptoms are not explained by an initial CT scan receive further investigations. If a patient presents with “red flag” symptoms such as a new seizure, persistent morning headache, or a progressive change in personality a negative CT scan is not considered the end of the diagnostic journey.
The UK follow-up pathway involves:
- Clinical Review: Re-evaluating the patient’s symptoms if they do not resolve.
- Specialist Referral: A GP referring the patient to a neurologist or neurosurgeon.
- Urgent MRI: Scheduling a detailed MRI scan, often under the 28-day faster diagnosis standard.
- MDT Discussion: A board of experts reviewing the clinical history and all imaging results.
This structured system acts as a safety net, ensuring that tumours that are difficult to see on a CT are eventually caught through more sensitive technology. Following these national protocols allows the NHS to maintain a high level of diagnostic accuracy. By coordinating care across different specialities, the UK ensures that patient safety is prioritised and that the most effective imaging tools are used at the right time in the patient’s clinical journey.
Conclusion
While a CT scan can detect many brain tumours, especially those that are large or cause significant pressure, it is not sensitive enough to identify every growth. Slow-growing or small tumours may look similar to healthy brain tissue on a CT, and bone interference can hide masses at the base of the skull. In the UK, the NHS uses CT for rapid emergency triage but relies on MRI as the gold standard for a definitive and detailed diagnosis. Consistent clinical monitoring and following the recommended diagnostic pathway are essential for ensuring an accurate assessment of neurological symptoms. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is a CT scan safe for children?
UK clinicians are extra cautious with children because CT scans use ionising radiation, so they only perform them when absolutely necessary or use MRI instead.
Can a CT scan tell the difference between a tumour and a stroke?
Yes, CT is very effective at quickly distinguishing between a brain haemorrhage (stroke) and a large tumour mass.
Why did I have a CT if I needed an MRI anyway?
A CT is often done first to rule out immediate life-threatening issues because it is much faster and more widely available than an MRI.
What happens if I can’t have an MRI due to a pacemaker?
If an MRI is not possible, UK specialists may use a contrast-enhanced CT scan or a specialised PET scan to get more information.
How long does a CT scan of the head take?
The actual scanning process in the UK usually takes less than five minutes, though the entire appointment may take longer.
Do I have to go inside a tunnel for a CT scan?
A CT scanner is shaped like a large ring or doughnut and is much more open than a traditional MRI tunnel, making it easier for people with claustrophobia.
Does a normal CT scan mean I definitely don’t have a tumour?
Not necessarily; if your symptoms continue, you should return to your GP, as a CT can miss certain small or slow-growing tumours.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding CT scans and brain tumours, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in emergency care, surgery, and clinical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
