Severe newborn jaundice can increase the risk of cerebral palsy if high levels of bilirubin are left untreated and cross into the brain, causing permanent damage to the motor control centres. In the United Kingdom, the NHS monitors all newborn infants for signs of jaundice to ensure early detection and treatment through phototherapy. While mild jaundice is common and usually harmless, identifying the rare progression to kernicterus is essential for protecting neurological health.
What We’ll Discuss in This Article
- The biological relationship between bilirubin levels and brain health.
- Understanding kernicterus as a preventable cause of brain injury.
- Identifying the clinical signs of severe jaundice in newborns.
- How the NHS utilises phototherapy and exchange transfusions.
- The specific type of cerebral palsy associated with jaundice.
- Integrated long-term monitoring and support within the UK.
The Biological Relationship Between Bilirubin and the Brain
Jaundice occurs when there is a buildup of bilirubin in the blood, a yellow substance produced when red blood cells are broken down, which can become toxic to the brain if levels rise excessively. Most newborns develop mild jaundice as their young livers begin to process bilirubin independently. The NHS states that in very rare cases, if jaundice is not treated and bilirubin levels become extremely high, it can lead to permanent brain damage.
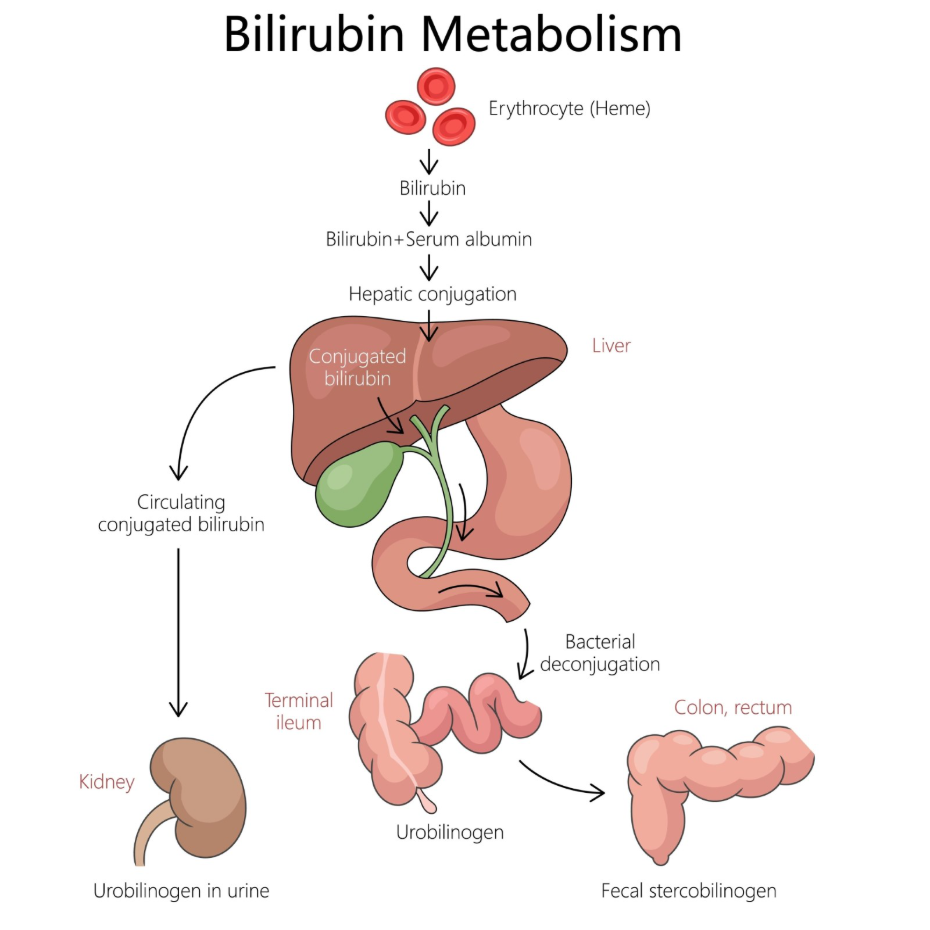
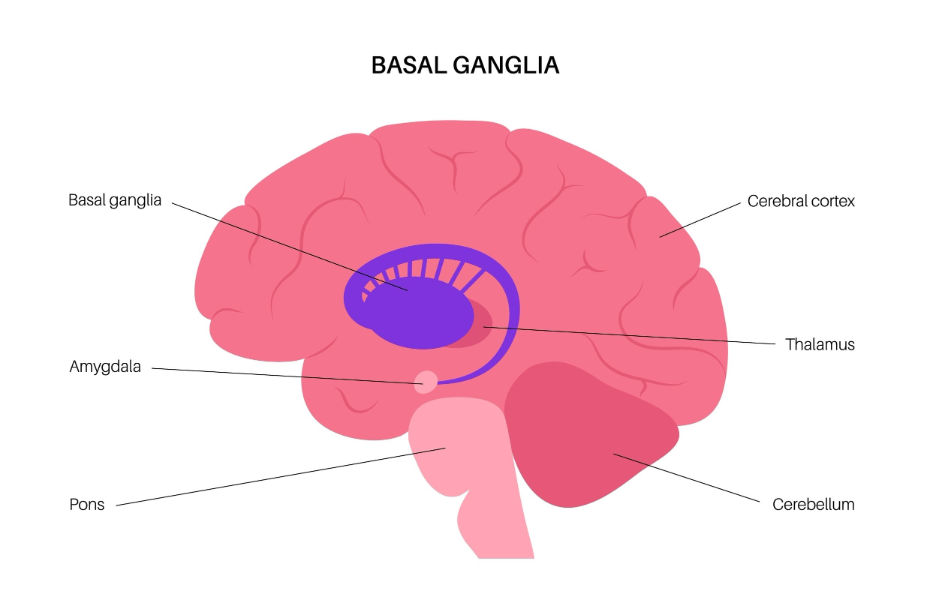
The primary risk involves “unconjugated” bilirubin, which is fat-soluble and can cross the blood-brain barrier if it reaches critical concentrations. Once in the brain, it has a particular affinity for the basal ganglia, the region responsible for smoothing out and coordinating voluntary movements. In the United Kingdom, midwives and neonatal teams use “bilirubin charts” to determine when an infant’s level is too high for their age and weight. By intervening before bilirubin reaches these dangerous thresholds, the healthcare system aims to prevent the neurological complications associated with jaundice. This structured monitoring is a cornerstone of UK neonatal safety, providing a clear pathway from initial screening to clinical intervention.
Understanding Kernicterus as a Preventable Injury
Kernicterus is the clinical term used in the United Kingdom for the permanent brain damage caused by excessive bilirubin levels, and it is considered a largely preventable cause of cerebral palsy. When bilirubin stains and damages the brain tissue, it results in a specific neurological profile often involving involuntary movements and hearing loss. NICE clinical guidelines for jaundice in newborns indicate that the primary goal of treatment is to prevent bilirubin encephalopathy and the subsequent development of kernicterus.
In the UK, the focus is on “timely treatment” to stop the transition from standard jaundice to acute bilirubin encephalopathy. Early signs that the brain is being affected include the baby becoming very sleepy, having a high-pitched cry, or arched-back posturing. If these signs are identified, the NHS initiates intensive treatment to lower bilirubin levels rapidly. Because kernicterus is a static injury, the resulting motor challenges will not worsen over time, but they require lifelong management. The UK healthcare framework emphasises that robust screening and parent education are the most effective tools for ensuring that this rare but serious complication is avoided.
Identifying Clinical Signs of Severe Jaundice
Identifying the clinical signs of worsening jaundice is a priority for healthcare professionals and parents in the United Kingdom to ensure that infants receive a bilirubin test at the earliest opportunity. While a yellowing of the skin and the whites of the eyes is typical, certain patterns suggest that the bilirubin level may be rising to a concerning degree.
Common signs of concern in the UK include:
- Rapid Progression: Yellowing that moves quickly from the face down to the chest and legs.
- Persistent Jaundice: Jaundice that appears within the first 24 hours of life or persists beyond two weeks.
- Behavioural Changes: The baby becoming difficult to wake or too tired to feed effectively.
- Dark Urine and Pale Stools: Potential indicators of underlying liver or biliary issues.
| Feature | Mild Jaundice (Common) | Severe Jaundice (Risk) |
| Appearance | Slight yellowing of face/chest. | Intense yellow/orange skin on limbs. |
| Feeding | Baby wakes and feeds well. | Baby is lethargic and lacks interest. |
| Timing | Starts 2 to 3 days after birth. | Starts within 24 hours of birth. |
| Muscle Tone | Normal and active movements. | Floppiness or stiff, arched back. |
In the United Kingdom, the “visual check” is always followed by a formal measurement if there is any doubt about the severity. This may involve a “bilirubinometer,” which uses light on the skin, or a blood test known as a “split bilirubin” test. These measurements are essential for determining if the baby needs to stay in hospital for treatment. The NHS provides clear guidance for parents on how to check their baby’s skin in natural light, ensuring that the safety net of monitoring extends from the hospital into the home.
NHS Treatments: Phototherapy and Exchange Transfusion
The United Kingdom utilises phototherapy as the primary treatment for lowering bilirubin levels, using specific blue light to break down the bilirubin in the skin so it can be excreted more easily. This non-invasive treatment is highly effective and has significantly reduced the number of infants at risk of developing kernicterus and cerebral palsy.
The treatment pathway in the UK involve:
- Standard Phototherapy: The baby is placed under one or more lamps with their skin exposed.
- Bili-blankets: Fibre-optic pads that can be used to provide light therapy while the baby is being held.
- Intensive Phototherapy: Using multiple light sources and increasing the surface area exposed.
- Exchange Transfusion: A specialist procedure where the baby’s blood is slowly replaced with donor blood to remove bilirubin rapidly.
Exchange transfusion is reserved for emergency situations where bilirubin levels are exceptionally high or not responding to light therapy. In the UK, this procedure is performed in specialist neonatal intensive care units (NICUs). By using these integrated treatments, the NHS aims to reduce the bilirubin load before it can cause neurological injury. Following treatment, the baby’s levels are monitored to ensure they do not rise again. This proactive medical management is essential for protecting the vulnerable neonatal brain from the toxic effects of chemical imbalances.
Dyskinetic Cerebral Palsy and Jaundice
The specific type of cerebral palsy typically caused by kernicterus is dyskinetic cerebral palsy, which is characterised by involuntary, uncontrolled movements and often associated with a specific type of hearing loss. This occurs because the bilirubin damage is concentrated in the basal ganglia, which is the part of the brain that regulates the smoothness and coordination of physical actions. The GOV.UK health pages provide clinical profiles indicating that the management of dyskinetic movements and sensory impairments is a priority for integrated neuro-disability services.
Symptoms of dyskinetic cerebral palsy in the UK include:
- Athetosis: Slow, writhing movements of the hands and feet.
- Chorea: Sudden, jerky motions that occur without intent.
- Dystonia: Twisting or repetitive movements caused by fluctuating muscle tone.
- Sensory-Neural Hearing Loss: Difficulty processing sound due to damage to the auditory pathways.
In the United Kingdom, children with this form of the condition are supported by a multidisciplinary team including speech and language therapists and audiologists. Because intelligence is often unaffected, the focus is on providing communication aids and postural support to help the individual express themselves and move as independently as possible. Understanding the specific link to jaundice helps UK clinicians provide an accurate prognosis and tailor the therapy to the person’s unique movement profile. The NHS ensures that these individuals have access to the full range of expertise required to manage the complex motor and sensory challenges associated with bilirubin-led injury.
Integrated Monitoring and Long-term Support
The United Kingdom provides a comprehensive framework of integrated support to monitor infants who have experienced severe jaundice and to provide long-term care for those who develop neurological complications. This coordinated effort ensures that any developmental delays are identified and addressed through a structured management plan.
The UK support framework involves:
- Neonatal Follow-up: Regular clinical reviews for infants who required intensive jaundice treatment.
- Audiology Screening: Specific tests to check for the hearing loss often associated with kernicterus.
- Physiotherapy Assessment: Monitoring for early signs of involuntary movement or tonal changes.
- Specialist Nursing Support: Providing a consistent point of contact for families during and after treatment.
This integrated approach ensures that the child’s progress is viewed holistically across different medical specialities. In the UK, the “Red Book” is used to track these reviews and ensures that the history of severe jaundice is known to all future healthcare providers. The healthcare system also provides transition services to help young people move from paediatric to adult neurology and therapy teams. By utilising this comprehensive safety net, the NHS aims to empower families and ensure that every individual impacted by jaundice-related challenges has the opportunity to achieve their functional potential.
Conclusion
Severe jaundice can increase the risk of cerebral palsy by causing bilirubin-related brain damage known as kernicterus. In the UK, the NHS manage this risk through routine screening and effective treatments like phototherapy to lower bilirubin levels before they become toxic. While mild jaundice is a normal part of newborn life, identifying red-flag signs like lethargy and rapid yellowing is essential for prevention. If brain injury occurs, it typically results in dyskinetic cerebral palsy, which requires lifelong multidisciplinary support. Following a structured management plan ensures that any developmental or sensory needs are addressed promptly. The UK healthcare system provides a life-long framework of support for children and their families.
Does every baby with jaundice need treatment in the UK?
No; most babies have mild jaundice that resolves on its own, but the NHS monitors all babies to see if treatment is required.
Can I prevent my baby from getting jaundice?
Frequent feeding in the first few days helps the baby pass bilirubin through their stools, which can help keep levels lower.
Is phototherapy painful for the baby?
No; phototherapy is a painless light treatment, though the baby will need to wear eye protection to stay comfortable under the lamps.
What is the “split bilirubin” blood test?
It is a test used in the UK to see how much bilirubin is “conjugated” versus “unconjugated,” helping doctors find the cause of the jaundice.
Can jaundice cause cerebral palsy if it starts after a week?
Jaundice that starts later is usually less risky for the brain, but it still requires a medical review to check for liver or biliary issues.
Why does jaundice cause hearing loss?
High bilirubin levels can damage the auditory nerve and the parts of the brain that process sound, alongside the motor control centres.
Who should I call if my jaundiced baby is not feeding?
In the UK, you should contact your midwife, GP, or NHS 111 immediately if your baby becomes lethargic or refuses feeds.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the link between jaundice and cerebral palsy, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in general surgery, cardiology, and emergency medicine. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
