Haemorrhoids, commonly referred to as piles, are swollen veins located in the lower rectum and anus that can cause discomfort, itching, or bleeding during bowel movements. They are a common physiological occurrence and are essentially analogous to varicose veins, developing when the blood vessels in the anal canal become enlarged and congested. While often associated with significant discomfort, they are generally manageable through lifestyle modifications and over-the-counter treatments, though persistent or severe cases may require a professional clinical review to exclude other underlying conditions.
What We’ll Discuss in This Article
- The biological structure and types of haemorrhoids
- Common lifestyle and physiological causes of vein swelling
- Recognising the typical symptoms and when they occur
- Standard management strategies and dietary adjustments
- Clinical procedures for persistent or severe cases
- Identifying red flag symptoms that require medical investigation
The Biological Structure and Classification of Haemorrhoids
Haemorrhoids are vascular cushions that exist naturally in the anal canal to assist with stool control, but they become a clinical issue only when they swell or become inflamed. These cushions are made of a network of small blood vessels, connective tissue, and smooth muscle. Depending on their location relative to the dentate line (the junction between the rectum and the anus), they are classified as either internal or external.
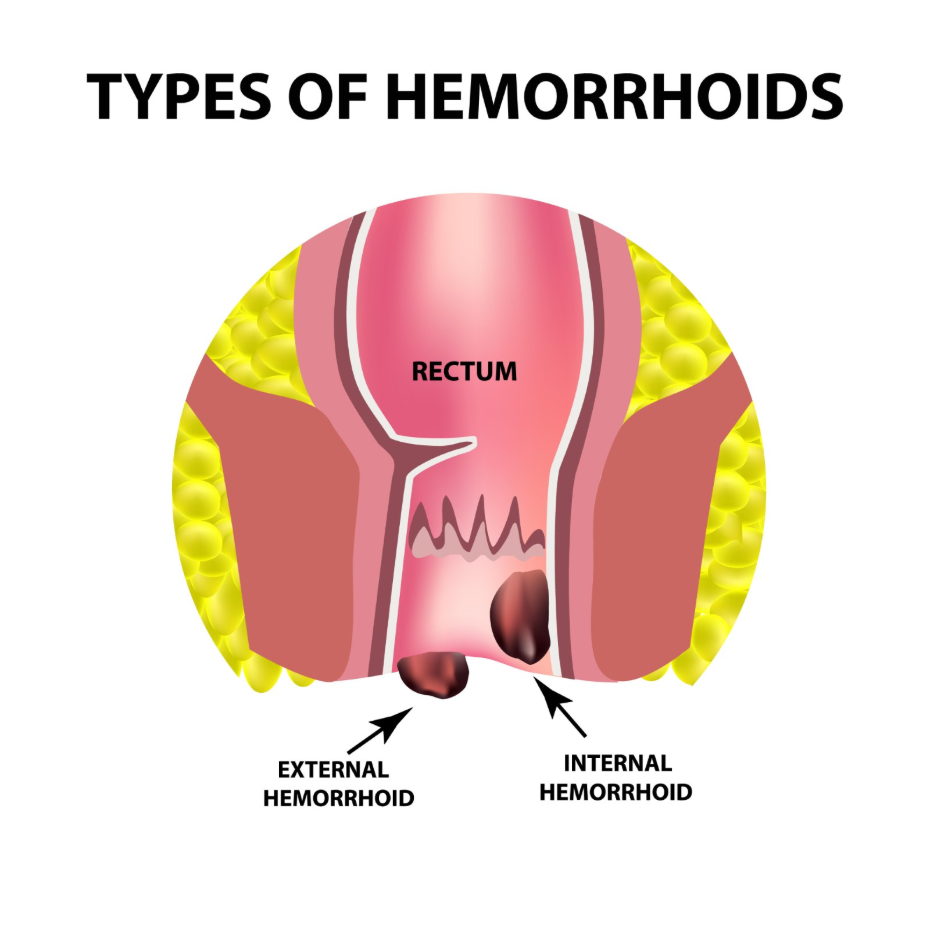
Internal haemorrhoids develop inside the rectum and are usually not visible or painful because there are few pain-sensing nerves in that area. However, they may bleed during a bowel movement or prolapse, which means they extend outside the anal opening. External haemorrhoids form under the skin around the anus, where there are many pain receptors. If a blood clot forms within an external haemorrhoid, it is known as a thrombosed haemorrhoid, which can cause significant swelling and acute pain. Haemorrhoids are swollen veins in the anus and lower rectum, similar to varicose veins, and they can develop inside the rectum or under the skin around the anus.
Common Causes and Risk Factors
The primary cause of haemorrhoids is increased pressure in the lower rectum, which causes the blood vessels to stretch and bulge. This pressure is most frequently the result of straining during bowel movements, often due to chronic constipation or diarrhoea. When the body exerts excessive force to pass hard stools, the vascular cushions become engorged and can eventually lose their supportive connective tissue, leading to displacement or swelling.
Other physiological factors also contribute to the development of piles. Pregnancy is a common trigger because the growing uterus exerts pressure on the veins in the pelvis, and hormonal changes can soften the vein walls. Ageing is another significant risk factor, as the tissues that support the veins in the rectum and anus can weaken and stretch over time. Additionally, lifestyle factors such as a low-fibre diet, obesity, and prolonged periods of sitting on the toilet can increase the likelihood of developing symptomatic haemorrhoids.
Recognising Typical Symptoms
Typical symptoms of haemorrhoids include painless bleeding during bowel movements, itching or irritation in the anal region, and a lump or swelling near the anus. Many patients first notice bright red blood on the toilet paper or in the toilet bowl after passing a stool. Because internal haemorrhoids lack pain fibres, the bleeding is often the only indicator of their presence unless they prolapse and cause a feeling of fullness.
External haemorrhoids are more likely to cause physical discomfort and itching because the skin in that area is highly sensitive. If an external haemorrhoid becomes thrombosed, the pain can be sharp and persistent, often making it difficult to sit or walk comfortably. The symptoms of piles often include bright red blood after you poo, an itchy anus, and feeling like you still need to poo after going to the toilet. While these symptoms are characteristic of haemorrhoids, they can overlap with other conditions, so a clinical assessment is important if symptoms are new or changing.
Management Strategies and Lifestyle Adjustments
Most cases of haemorrhoids can be managed effectively through dietary changes and habits that aim to soften the stool and reduce pressure on the anal veins. Increasing the intake of dietary fibre is the most important step, as it adds bulk to the stool and makes it easier to pass without straining. Recommended sources of fibre include whole grains, legumes, fruits, and vegetables. It is essential to increase fibre intake gradually and pair it with adequate hydration to prevent further constipation.
In addition to diet, specific bathroom habits can significantly reduce symptoms. Avoiding the urge to strain and limiting the amount of time spent sitting on the toilet can prevent unnecessary pressure on the rectal veins. Over-the-counter treatments, such as creams, ointments, or suppositories containing local anaesthetics or mild corticosteroids, can provide temporary relief from itching and swelling. The National Institute for Health and Care Excellence provides guidelines on the management of haemorrhoids, emphasising the importance of fibre and lifestyle changes as a first-line approach.
Clinical Procedures for Persistent Cases
If lifestyle modifications and over-the-counter treatments do not resolve the symptoms, various non-surgical and surgical procedures may be considered. Rubber band ligation is a common non-surgical treatment for internal haemorrhoids where a small band is placed around the base of the haemorrhoid to cut off its blood supply, causing it to wither and drop off. Sclerotherapy is another option, involving the injection of a chemical solution into the haemorrhoid tissue to shrink it.
For more severe, persistent, or prolapsed haemorrhoids, surgical interventions may be necessary. A haemorrhoidectomy is the surgical removal of the haemorrhoid tissue and is typically reserved for large or recurring cases. Another technique, haemorrhoid stapling, involves repositioning the prolapsed tissue and cutting off the blood supply. These procedures are usually performed by a specialist surgeon and require a period of recovery and specific post-operative care to ensure long-term resolution of the symptoms.
When to Seek Medical Investigation
While haemorrhoids are a common cause of rectal bleeding, it is vital to have any new or persistent bleeding assessed by a healthcare professional to rule out more serious conditions. Bleeding from the rectum can also be a symptom of inflammatory bowel disease or colorectal cancer, particularly in older individuals or those with a family history of such conditions. A clinical assessment ensures that the diagnosis is accurate and that the appropriate treatment pathway is followed.
Red flag symptoms that require a professional review alongside suspected haemorrhoids include:
- A persistent change in bowel habit lasting more than three weeks
- Unintentional and unexplained weight loss
- Severe abdominal pain or a feeling of incomplete evacuation
- Bleeding that is dark in colour or mixed with mucus
- A lump in the anal area that is hard, persistent, or extremely painful
Healthcare providers may use a physical examination, including a digital rectal exam, or a proctoscopy to visualise the anal canal and confirm the presence of haemorrhoids. If there are concerns about the upper colon, a referral for a colonoscopy may be necessary.
Conclusion
Haemorrhoids are a common and generally benign condition caused by increased pressure on the veins in the rectal and anal area. Most symptoms can be managed through a high-fibre diet, increased fluid intake, and improved bathroom habits. However, persistent symptoms or any form of rectal bleeding should be evaluated by a healthcare professional to confirm the cause and ensure digestive health is maintained. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can haemorrhoids be prevented?
Yes, maintaining a high-fibre diet, drinking plenty of water, and avoiding straining during bowel movements are effective ways to prevent the development of piles.
Are haemorrhoids the same as bowel cancer?
No, they are entirely different conditions; haemorrhoids are swollen veins, while cancer is a growth of abnormal cells, though both can cause rectal bleeding.
Do haemorrhoids go away on their own?
Many mild haemorrhoids will shrink and resolve within a few days of improving diet and habits, though some may recur or require medical treatment.
Is it safe to use over-the-counter creams for a long time?
Most over-the-counter haemorrhoid creams containing steroids should only be used for a maximum of seven days to avoid thinning the skin in the anal area.
Can exercise help with haemorrhoids?
Gentle exercise like walking helps maintain regular bowel movements and reduces pressure on the veins, but heavy lifting can sometimes worsen symptoms.
What is a thrombosed haemorrhoid?
This occurs when a blood clot forms in an external haemorrhoid, causing a hard, painful lump that may require a minor procedure to drain.
Does sitting on cold surfaces cause piles?
No, there is no clinical evidence to support the theory that sitting on cold surfaces causes haemorrhoids; they are primarily caused by internal pressure.
Authority Snapshot (E-E-A-T)
This medical education content is designed to provide accurate, evidence-based information for the UK public regarding haemorrhoids. The material is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience across internal medicine, general surgery, and acute care. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
