Constipation is the leading cause of anal fissures, as the passage of hard or unusually large stools can easily overstretch and tear the delicate lining of the anal canal. This mechanical trauma occurs when the mucosal tissue is forced to expand beyond its elastic capacity, resulting in a small cut or split. While the injury itself is often small, the high density of nerves in the area ensures that the resulting pain is sharp and intense. Understanding how bowel habits influence the integrity of the anal lining is an essential part of managing current symptoms and preventing the recurrence of these painful tears through dietary and lifestyle modifications.
What We’ll Discuss in This Article
- The physiological link between hard stools and mucosal tearing
- How straining during bowel movements increases the risk of injury
- The impact of chronic constipation on the healing of existing fissures
- Dietary strategies to soften stools and reduce mechanical friction
- The role of hydration and fibre in maintaining a healthy anal canal
- When to seek professional medical advice for persistent symptoms
Mechanical Trauma and the Formation of a Tear
Constipation causes anal fissures primarily through the direct physical trauma of passing waste that is too firm, dry, or large for the anal canal to accommodate comfortably. When waste material remains in the colon for an extended period, the body reabsorbs excessive amounts of water, leading to stools that are compact and lose their natural lubrication. As these stools are expelled, they exert significant pressure against the thin, moist tissue that lines the anus, known as the anoderm.
If the tissue is subjected to more force than it can withstand, a linear tear or split forms, most commonly at the back of the anal opening. An anal fissure is a small tear in the lining of the anus that is most often caused by the passage of very hard or large stools during a bout of constipation. This injury is often felt immediately as a sharp, stinging sensation. Because the anal canal is designed to stay closed to maintain continence, any stool that requires the canal to open wider than usual puts the lining at risk of mechanical failure.
The Impact of Straining on the Anal Canal
Straining to pass a bowel movement significantly increases the likelihood of developing an anal fissure by placing acute vascular and mechanical stress on the anal lining. When an individual “bears down” or uses force to empty their bowels, the internal pressure within the rectum and anal canal spikes. This pressure not only engorges the blood vessels but also pulls the mucosal tissue taut, making it more brittle and susceptible to cracking under the friction of the stool.
Repeated straining can also lead to an increase in the resting tone of the internal anal sphincter muscle. If this muscle becomes too tight or begins to spasm as a result of the effort, it restricts blood flow to the anal lining. The National Institute for Health and Care Excellence notes that constipation and the associated straining are the primary triggers for acute anal fissures in both adults and children. Without adequate blood flow, the tissue loses its resilience, making it even more likely to tear during the next episode of constipation, thereby creating a cycle of injury and poor healing.
How Constipation Prevents Natural Healing
Persistent constipation is the most common factor that prevents an acute anal fissure from healing, often causing it to become a chronic, non-healing wound. For a tear to knit back together, the area needs to remain undisturbed and have an adequate blood supply. However, every time a hard stool is passed, it re-opens the healing edges of the fissure, effectively resetting the recovery timeline. This repeated mechanical disruption ensures the wound remains raw and sensitive.
Furthermore, the pain associated with passing hard stools over a fissure can lead to “toilet avoidance,” where an individual subconsciously delays going to the bathroom. This delay allows the stool to sit in the rectum even longer, becoming harder and more difficult to pass, which worsens the constipation. The symptoms of an anal fissure, including sharp pain and bright red bleeding, often persist if the underlying constipation is not effectively managed through lifestyle changes. Breaking this cycle requires a consistent effort to maintain soft stools so that the anal lining can remain intact for several weeks of uninterrupted healing.
Dietary Strategies for Preventing Tears
Managing constipation through dietary adjustments is the most effective way to prevent the formation of anal fissures and support the repair of existing ones. A diet rich in fibre is essential for adding bulk to the stool and retaining moisture, which ensures the waste material passes smoothly through the anal canal. Fibre acts as a natural sponge, preventing the waste from becoming the hard, abrasive lumps that cause mechanical trauma.
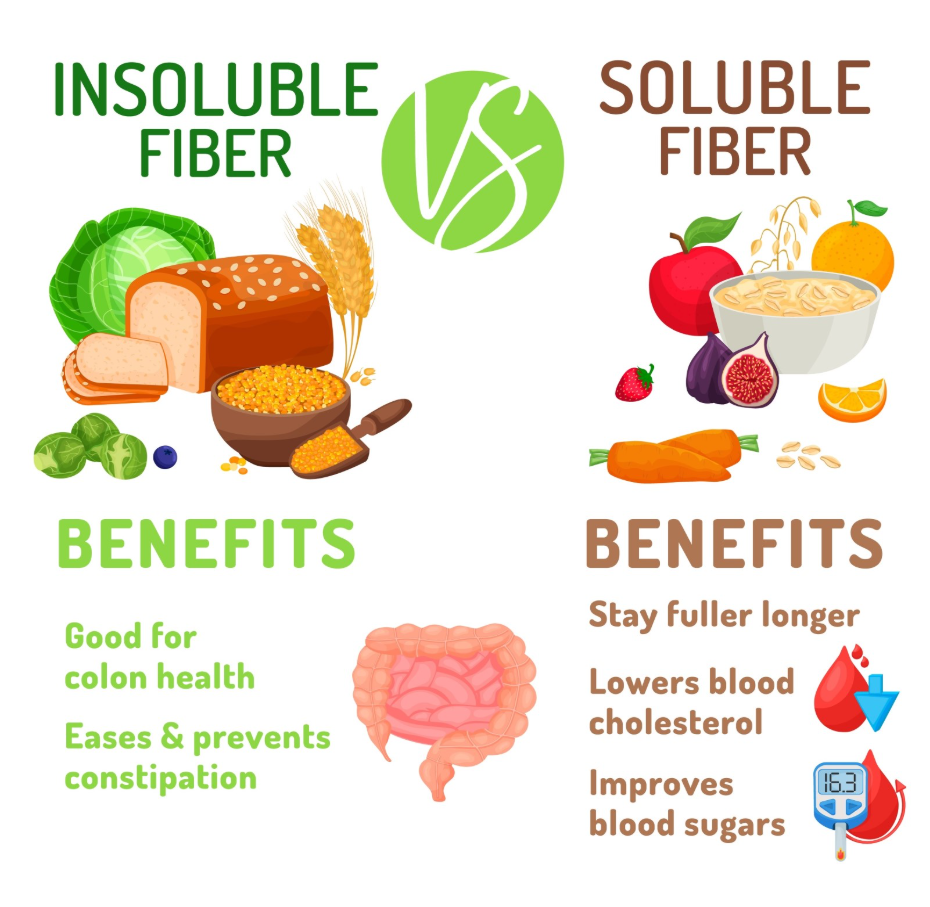
Individuals should focus on incorporating a variety of fibre sources, such as whole grains, pulses, and leafy green vegetables. It is generally recommended to increase fibre intake gradually to allow the digestive system to adapt without causing excess gas or bloating. Consuming fruits like prunes, pears, and apples with their skins on provides both soluble and insoluble fibre, which are vital for maintaining a healthy digestive transit time and reducing the need for the straining that causes fissures.
The Relationship Between Fibre and Hydration
Fibre can only prevent the constipation that causes fissures if it is accompanied by a significant intake of fluids. Without adequate water, a high-fibre diet can actually make constipation worse by creating stools that are too bulky and dry to move efficiently. Water ensures that the fibre remains soft and pliable as it travels through the colon, allowing the stool to slide easily over the sensitive anal lining without causing friction.
Most adults in the United Kingdom are advised to drink at least six to eight glasses of fluid a day, ideally focusing on water. During a fissure flare-up, staying well-hydrated is a clinical priority to minimise the pain associated with daily bowel movements. Avoiding excessive caffeine or alcohol is also helpful, as these substances can have a dehydrating effect on the body, potentially leading to the very constipation that individuals are trying to avoid.
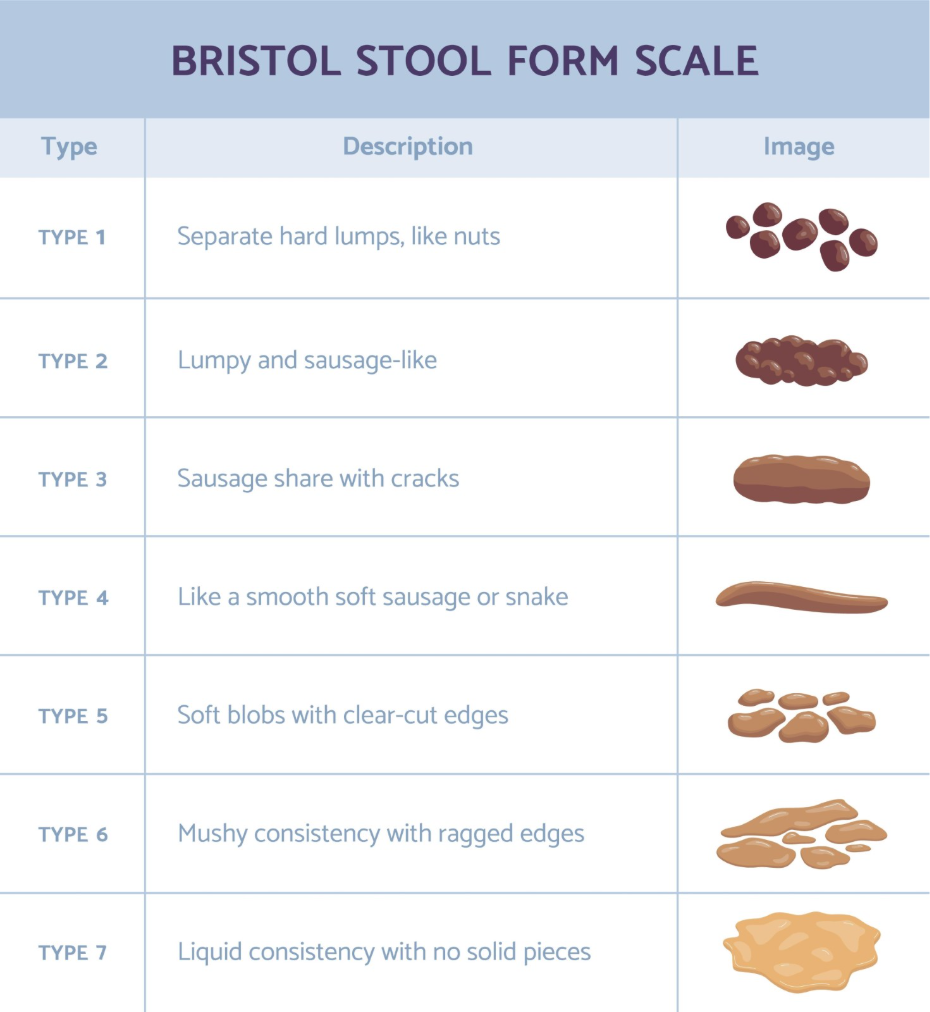
Comparing Stool Consistency and Fissure Risk
The following table demonstrates how stool consistency, as classified by clinical standards, impacts the physical risk to the anal lining.
| Stool Type | Characteristics | Impact on Anal Fissure |
| Hard/Lumpy | Small, dry, and difficult to pass | Very High: Causes mechanical tearing |
| Soft/Formed | Sausage-shaped with some cracks | Low: Passes easily with minimal stretching |
| Smooth/Soft | Soft and easy to pass (like a banana) | Ideal: Allows the tissue to heal |
| Liquid/Loose | Entirely liquid or soft blobs | Moderate: Can cause chemical irritation |
When to Seek a Professional Medical Review
While many fissures caused by temporary constipation heal within a few weeks, a medical review is necessary if the pain is severe or if symptoms do not improve. A healthcare professional can confirm the diagnosis and provide access to medicated treatments that help the anal muscles relax, which is often required if constipation has caused a chronic tear. In the UK, GPs follow structured protocols to ensure that symptoms are correctly managed and that any underlying conditions are investigated.
Professional advice should be sought if:
- The pain during or after bowel movements is preventing you from eating or going to the toilet
- Rectal bleeding is heavy, dark in colour, or mixed within the stool
- You experience a persistent change in bowel habit lasting three weeks or more
- You notice a hard lump or swelling near the site of the pain
- You experience unintentional weight loss or severe abdominal cramping
A clinician may recommend over-the-counter bulk-forming laxatives to help manage the constipation while the fissure heals. These are designed to supplement dietary fibre and ensure that the stool consistency remains optimal for tissue repair.
Conclusion
Constipation is the primary cause of anal fissures due to the mechanical stress and trauma associated with passing hard stools and straining. These actions lead to a tear in the sensitive anal lining, which can become chronic if the underlying bowel habits are not corrected. By focusing on a high-fibre diet, proper hydration, and gentle hygiene, most individuals can manage constipation-related fissures effectively at home. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why does my fissure only hurt when I am constipated?
The pain is caused by the stool stretching the tear; when you are not constipated, the stool is soft enough to pass without reopening or irritating the injury.
Can I use laxatives to help my fissure heal?
Bulk-forming laxatives are often recommended to keep stools soft, but you should consult a pharmacist or GP before using them for an extended period.
Does a single episode of constipation always cause a fissure?
Not always, but if the stool is particularly hard or large, a single episode of straining can be enough to cause an acute tear in the anal lining.
Will my fissure come back if I get constipated again?
Yes, because the area where the original tear occurred may remain slightly more fragile, future bouts of constipation can easily cause a recurrence.
Why is water so important for a fissure?
Water keeps the stool soft and lubricated, which reduces the friction and force required to empty the bowels, protecting the anal lining from injury.
Can children get fissures from constipation?
Yes, anal fissures are a very common cause of rectal pain and bleeding in children, often resulting from a cycle of painful stools and “holding on.”
How much fibre do I need to prevent constipation?
In the UK, adults are encouraged to aim for 30g of fibre per day from a variety of plant-based sources to maintain healthy, soft stools.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information regarding the link between constipation and anal fissures. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
