Surgery for a chronic anal fissure carries a small, recognised risk of affecting bowel continence because certain procedures involve making a physical change to the muscles responsible for controlling the passage of gas and stool. While the vast majority of patients undergo surgery without long-term complications, the internal anal sphincter is a critical component of the body’s ability to maintain control. Most surgical interventions in the United Kingdom are only recommended after conservative and medicated treatments have failed to heal the tear. Understanding how these procedures interact with the anal muscles and the measures taken to minimise risks is essential for patients considering surgery as a definitive solution for persistent pain and non-healing fissures.
What We’ll Discuss in This Article
- The anatomical role of the anal sphincter in maintaining continence
- How lateral internal sphincterotomy impacts muscle function
- Distinguishing between temporary and permanent changes in control
- Clinical risk factors that influence surgical outcomes
- Alternative surgical techniques designed to preserve continence
- Post-operative expectations and monitoring in the UK health system
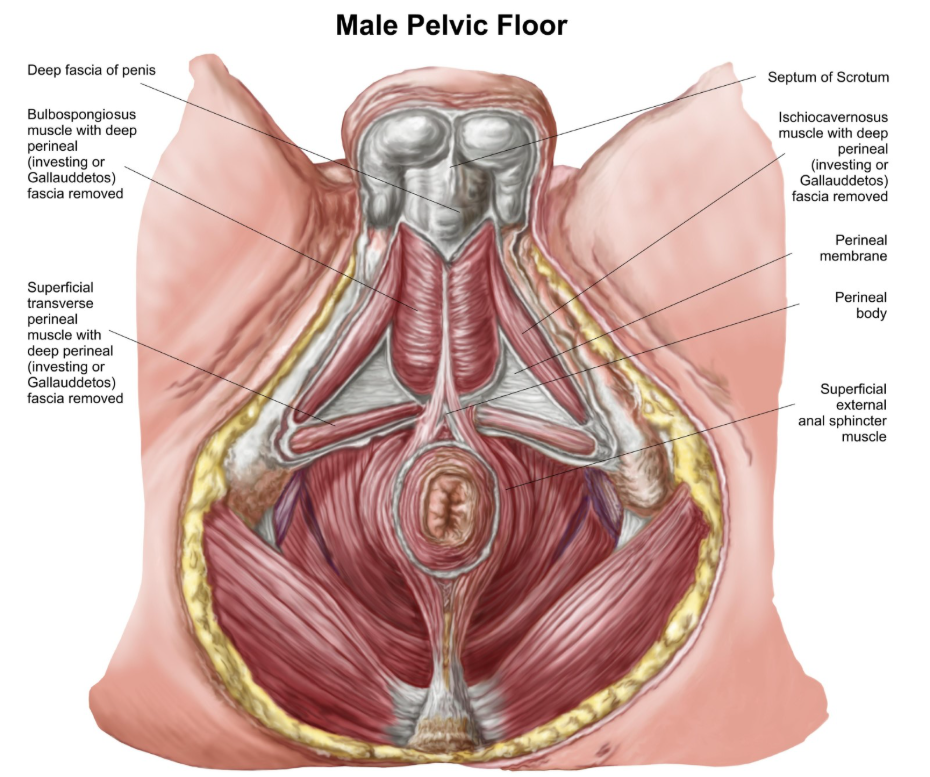
The Role of the Anal Sphincter in Continence
The anal sphincter complex consists of internal and external muscle rings that work together to maintain bowel control and prevent the involuntary passage of gas or stool. The internal anal sphincter is an involuntary smooth muscle that provides the majority of the resting pressure in the anal canal, keeping it closed at all times. The external anal sphincter is a voluntary muscle that a person can contract intentionally to delay a bowel movement.
When a fissure surgery is performed, it typically targets the internal sphincter to reduce the high resting pressure that prevents a tear from healing. An anal fissure is a small tear in the lining of the anus, and surgery may be considered if other treatments have not worked to relax the anal muscles. Because this muscle is vital for keeping the anal canal sealed, any surgical reduction in its strength has the potential to alter how effectively that seal is maintained. Clinicians carefully assess the existing strength of these muscles before proceeding with surgery to ensure that the patient has sufficient muscular reserve to maintain control after the procedure.
Lateral Internal Sphincterotomy and Continence Risks
Lateral internal sphincterotomy is the most common surgery for chronic fissures and involves a small cut in the internal muscle, which carries a statistically small but important risk of affecting continence. By partially dividing the internal sphincter, the surgeon permanently lowers the resting pressure in the anal canal. This allows blood flow to return to the site of the fissure, enabling the tissue to heal.
The National Institute for Health and Care Excellence notes that while lateral internal sphincterotomy is highly effective for healing fissures, it is associated with a small risk of minor incontinence to gas or liquid stool. In the majority of cases, this effect is minor and may involve difficulty distinguishing between gas and liquid or occasional slight staining of underwear. Severe loss of bowel control is very rare following modern surgical techniques. UK surgeons typically use a “tailored” approach, only cutting the minimum amount of muscle necessary to achieve healing while preserving as much continence function as possible.
Temporary vs Permanent Changes in Control
It is common for patients to experience temporary changes in bowel control immediately after fissure surgery, which often resolve as the surgical site heals and inflammation subsides. During the first few weeks post-operation, the area may be swollen, and the local nerves may be sensitive, which can temporarily affect the coordination of the sphincter muscles. This is often referred to as transient incontinence and is typically limited to the passage of wind or minor spotting.
Permanent changes are defined as those that persist beyond the initial healing period of six to twelve weeks. While the majority of patients find their control returns to normal once the fissure has healed and the soreness has gone, a small percentage may notice a lasting difference in their ability to hold gas. The symptoms of an anal fissure, such as sharp pain and bleeding, usually resolve quickly after surgery, but patients must discuss the potential long-term impact on muscle function with their consultant. Clinicians monitor patients during follow-up appointments to differentiate between normal post-operative recovery and any lasting changes that may require pelvic floor exercises or further management.
Clinical Risk Factors for Incontinence
Certain patient-specific factors can increase the risk of experiencing continence issues following fissure surgery, and these are carefully evaluated during the pre-operative assessment. Individuals who already have a degree of muscle weakness or those who have had previous anal surgeries may be at a higher risk. This is because their “functional reserve” the baseline strength of their sphincter complex is lower than average, making them more sensitive to the effects of a sphincterotomy.
| Risk Factor | Reason for Increased Risk |
| Previous Childbirth | Potential undiagnosed injury to the anal sphincter |
| Advanced Age | Natural age-related weakening of the pelvic floor muscles |
| Previous Anal Surgery | Existing scar tissue or previous muscle damage |
| Inflammatory Bowel Disease | Chronic inflammation can affect tissue and muscle integrity |
| Pre-existing Weakness | Baseline low resting pressure in the anal canal |
Surgeons may use specialised tests, such as anal manometry or ultrasound, to measure the pressure and integrity of the sphincter muscles before surgery if these risk factors are present. This allows the clinical team to determine if a muscle-cutting procedure is appropriate or if an alternative technique should be used to protect the patient’s long-term bowel control.
Continence-Preserving Surgical Alternatives
For patients at a higher risk of incontinence, alternative surgical procedures such as anal advancement flaps may be utilised to heal the fissure without cutting the sphincter muscle. This technique involves taking a small piece of healthy skin or mucosal tissue from near the anal opening and moving it to cover the chronic tear. Because the muscle is left intact, the risk of affecting bowel control is significantly lower than with a sphincterotomy.
Another option often explored before permanent surgery is the use of botulinum toxin injections. This provides a temporary “medical sphincterotomy” by paralysing a portion of the muscle for three to six months. While the effect is temporary, it often provides enough relaxation for the fissure to heal without the permanent structural changes associated with surgery. These alternatives are part of the standard UK clinical pathway to ensure that patients who are not suitable for traditional surgery still have access to effective treatments for chronic anal tears.
Comparison of Surgical Risks and Success
The following table compares the two primary surgical approaches in terms of their impact on healing and the risk to continence.
| Procedure | Success in Healing | Impact on Muscle | Continence Risk |
| Sphincterotomy | Very High (90%+) | Permanent incision | Recognised (mainly gas) |
| Advancement Flap | High (70-80%) | None (muscle preserved) | Very Low |
| Botox Injection | Moderate (60-70%) | Temporary relaxation | Very Low (reversible) |
Post-Operative Recovery and Long-Term Care
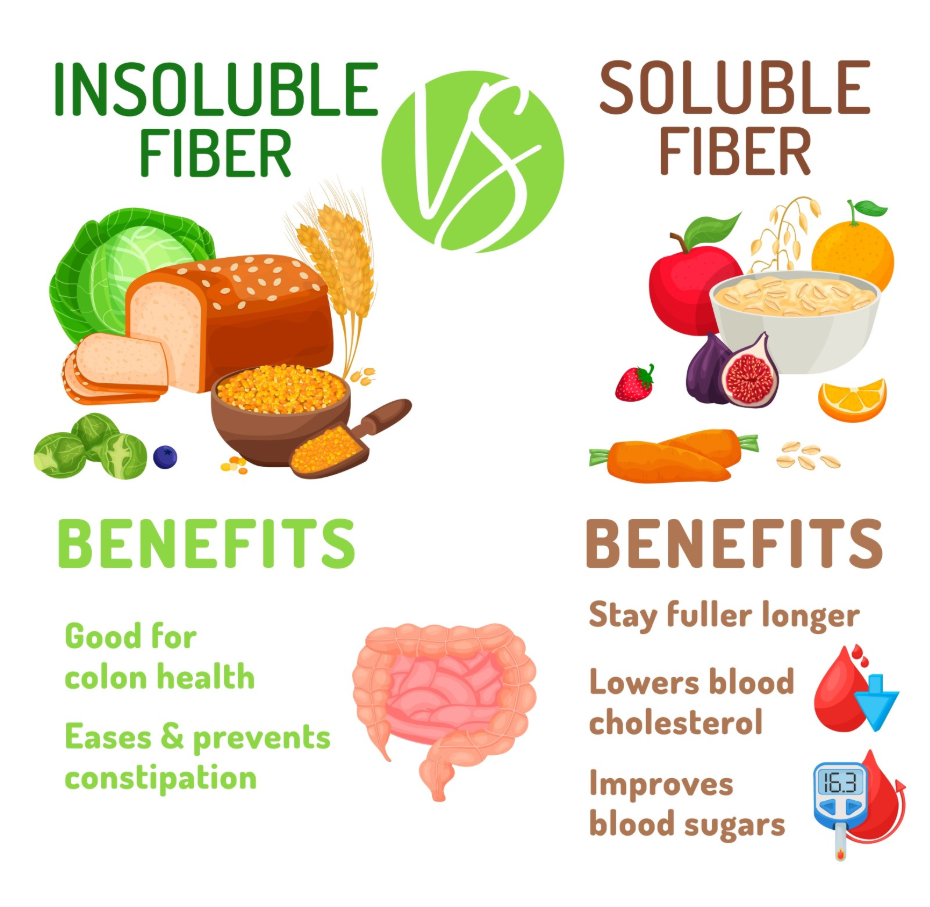
Following fissure surgery, the focus is on supporting the healing of the surgical site while maintaining healthy bowel habits to prevent future issues. Patients are advised to follow a high-fibre diet and drink plenty of water to ensure stools remain soft and pass without straining. Straining can put undue pressure on the healing muscles and the surgical incision, potentially complicating the recovery process.
If any minor changes in control are noticed during the recovery phase, simple measures such as pelvic floor muscle training may be recommended. These exercises help to strengthen the voluntary external anal sphincter, which can compensate for the changes made to the internal muscle. Most patients find that their quality of life improves significantly after surgery because the debilitating pain of the fissure is removed, allowing them to return to normal activities without the fear of painful bowel movements.
Conclusion
Fissure surgery, particularly lateral internal sphincterotomy, does carry a small risk of affecting continence, primarily related to the control of gas. This risk is managed through careful pre-operative assessment and the use of tailored surgical techniques that preserve as much muscle function as possible. While most patients experience a full recovery with improved quality of life, alternative procedures are available for those at higher risk of muscle weakness. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is the loss of bowel control common after fissure surgery?
No, significant loss of control is rare; most reported issues are minor, such as difficulty controlling wind or minor staining.
Will I be able to hold my bowels normally after a sphincterotomy?
The majority of patients maintain normal bowel control for stool, as the voluntary external sphincter remains fully functional.
Can pelvic floor exercises help if my continence is affected?
Yes, strengthening the external sphincter through regular exercises can often compensate for the reduced pressure of the internal muscle.
How do I know if I am at high risk for incontinence?
Your surgeon will assess factors such as your age, history of childbirth, and any previous surgeries to determine your individual risk level.
Is the effect on continence immediate after surgery?
You may notice minor changes early on due to swelling and soreness, but true assessment of continence happens after full healing.
Does botox cause permanent incontinence?
No, the effects of botulinum toxin are temporary and typically wear off within three to six months as the muscle regains its strength.
What should I do if I notice staining after surgery?
Keep the area clean and dry, use soft stool habits, and report any persistent issues to your surgical team during follow-up.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information regarding the risks of fissure surgery for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
