Pregnancy significantly increases the likelihood of developing haemorrhoids due to a combination of physiological pressure, hormonal fluctuations, and changes in digestive transit. Haemorrhoids, also known as piles, are swollen blood vessels in the rectum and anus that frequently become symptomatic during the second and third trimesters. While they can be uncomfortable and distressing, they are a common occurrence during the gestational period and often resolve or improve significantly following childbirth. Understanding the specific mechanisms that contribute to this risk allows expectant mothers to adopt preventative measures and manage symptoms effectively in line with clinical standards.
What We’ll Discuss in This Article
- The physical impact of the growing uterus on pelvic veins
- How progesterone influences vein walls and digestive speed
- The role of increased blood volume in vascular engorgement
- Managing pregnancy-related constipation to reduce straining
- Safe comfort measures for alleviating swelling and itching
- Clinical indicators for seeking advice from a midwife or doctor
Physical Pressure and Pelvic Venous Return
Pregnancy increases the risk of haemorrhoids primarily because the growing uterus places direct physical pressure on the pelvic veins and the inferior vena cava. As the foetus develops, the uterus expands and occupies more space within the pelvic cavity, which can partially obstruct the return of blood from the lower half of the body to the heart. This backup of blood causes the veins in the rectal and anal area to become congested and swollen, leading to the formation of haemorrhoids.
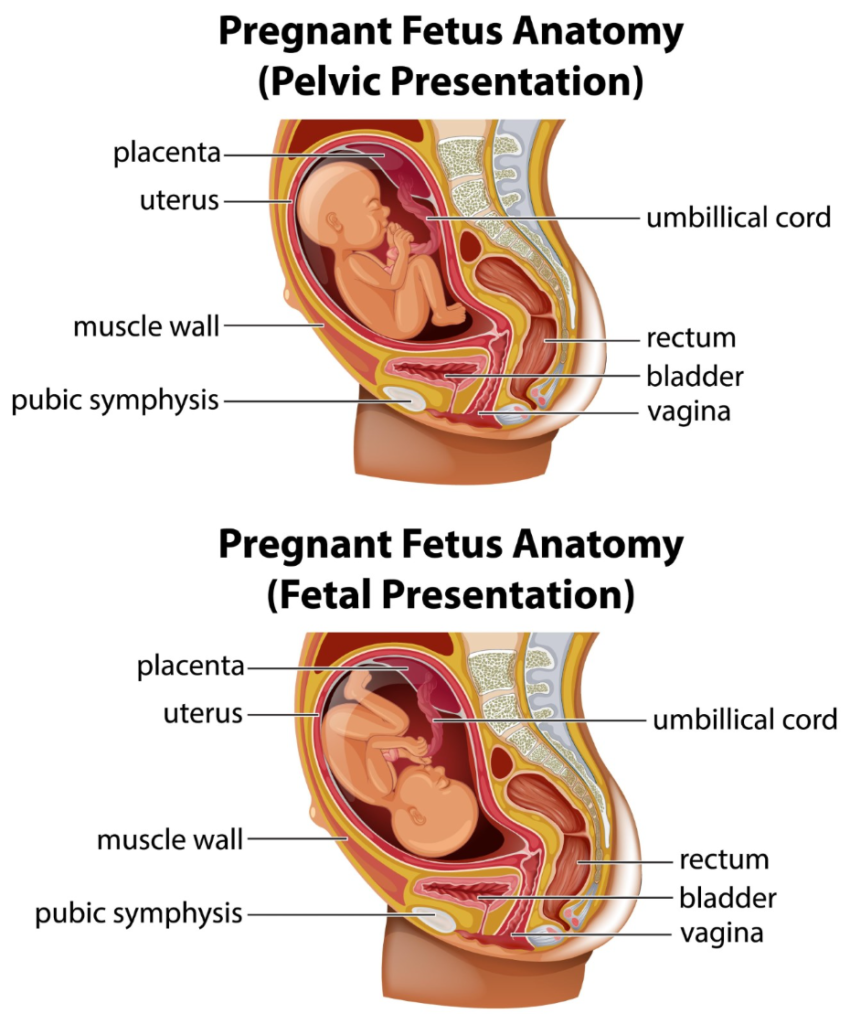
This pressure is often most acute during the third trimester when the weight of the baby is at its highest. Activities such as standing for long periods or sitting without adequate support can further impede blood flow, exacerbating the engorgement of these vascular cushions. Haemorrhoids are very common during pregnancy and often resolve or improve significantly after the baby is born. Maintaining positions that encourage circulation, such as lying on the left side, can help alleviate some of this direct mechanical pressure on the major vessels.
Hormonal Influence on Vein Walls and Digestion
The hormone progesterone, which rises significantly during pregnancy, causes the walls of the veins to relax and makes the digestive system more prone to constipation. Progesterone acts as a smooth muscle relaxant to prevent premature uterine contractions; however, this effect is not limited to the reproductive system. The muscles within the walls of the veins also relax, making them more susceptible to stretching and bulging under pressure.
Additionally, the relaxing effect of progesterone slows down the wave-like contractions of the intestines, known as peristalsis. This slower transit time allows the colon to reabsorb more water from waste material, often resulting in harder stools that are difficult to pass. Constipation is a common condition that can often be managed by making simple changes to your diet and lifestyle, such as increasing fibre and staying active. The resulting need to strain during bowel movements is a major secondary factor that causes haemorrhoids to flare up during pregnancy.
Increased Blood Volume and Vascular Engorgement
During pregnancy, the total volume of blood in the body increases by approximately forty to fifty percent to support the developing foetus and the placenta. This significant increase in circulatory volume places a general strain on the entire vascular system, particularly the veins in the lower extremities and the pelvic floor. Because veins are more distensible than arteries, they expand to accommodate the extra fluid, making the naturally occurring cushions in the anal canal larger and more prone to inflammation.
The combination of higher blood volume and the vasodilatory effects of pregnancy hormones means that even minor instances of straining can trigger rectal bleeding or swelling. This physiological state remains until after delivery, when the body begins to return to its pre-pregnancy fluid levels. Understanding that this is a systemic change helps clarify why haemorrhoids are so prevalent among expectant mothers, even those who may not have experienced digestive issues prior to pregnancy.
Managing Straining and Bathroom Habits
Reducing the amount of time spent straining on the toilet is a critical lifestyle modification for managing haemorrhoids during pregnancy. Midwives and healthcare professionals often recommend responding immediately to the urge to pass a bowel movement to prevent stool from becoming harder in the rectum. Using a small footstool to elevate the knees while sitting on the toilet can help align the rectum more effectively, allowing waste to pass with less physical effort and pressure on the anal veins.
It is also advised to avoid spending excessive time sitting on the toilet, such as when reading or using a mobile phone, as the unsupported position of the anus in this posture encourages blood to pool in the haemorrhoidal tissue. The National Institute for Health and Care Excellence provides guidelines for the management of haemorrhoidal disease, including advice for pregnant women on reducing straining and improving bowel habits. Simple changes to the mechanics of going to the toilet can prevent existing piles from becoming thrombosed or excessively painful.
Dietary Strategies for Softening Stool
A diet high in fibre and adequate fluid intake is essential for preventing the constipation that worsens pregnancy-related haemorrhoids. Expectant mothers are encouraged to gradually increase their intake of whole grains, pulses, fruits, and vegetables to ensure stools remain soft and bulky. Fibre requires significant amounts of water to function correctly; without enough hydration, a high-fibre diet can sometimes lead to further impaction.
| Food Category | Recommended Options | Benefit for Pregnancy |
| Whole Grains | Oats, brown rice, wholemeal bread | Provides consistent bulk to stool |
| Fruits | Apples, pears, berries, prunes | Natural sugars and fibre aid transit |
| Vegetables | Broccoli, carrots, leafy greens | High water and fibre content |
| Legumes | Lentils, chickpeas, beans | Significant fibre to reduce straining |
Staying active through gentle exercise, such as walking or prenatal swimming, also supports healthy gut motility. Movement helps the intestines process waste more efficiently, reducing the time that blood-congesting waste sits in the lower colon.
Safe Comfort Measures and Clinical Review
Managing the discomfort of pregnancy-related haemorrhoids often involves simple, non-medicinal comfort measures that can be used safely at home. Soaking the area in plain, warm water (a sitz bath) several times a day can help relax the anal sphincter and soothe irritated tissues. Patting the area dry gently with a soft towel rather than rubbing can prevent further skin breakdown and itching.
While many over-the-counter haemorrhoid creams are available, it is important to consult a pharmacist or midwife before using any medicated products during pregnancy. Some treatments contain ingredients that may not be suitable, so professional advice ensures that the chosen relief is safe for both the mother and the baby. A clinical review is necessary if there is significant rectal bleeding, severe pain, or if a lump becomes hard and bluish, which may indicate a blood clot.
Conclusion
Pregnancy increases the risk of haemorrhoids due to the direct pressure of the uterus on pelvic veins and the muscle-relaxing effects of progesterone. These factors, combined with increased blood volume and a tendency toward constipation, make vascular swelling in the anal canal very common. Most cases can be managed through dietary fibre, hydration, and improved bathroom habits, with many symptoms resolving after delivery. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why do haemorrhoids often appear in the third trimester?
The third trimester is when the uterus is at its heaviest, placing the maximum amount of pressure on the pelvic veins and the inferior vena cava.
Will my haemorrhoids go away after I give birth?
In many cases, the pressure is relieved after delivery and hormone levels stabilise, allowing the swollen veins to shrink and symptoms to subside.
Is it safe to use laxatives during pregnancy?
Bulk-forming laxatives are generally considered safe, but you must always consult your midwife or GP before taking any medication for constipation.
Can straining during labour make piles worse?
The intense pushing during the second stage of labour can cause existing haemorrhoids to swell or new ones to form, but this is usually temporary.
Does sleeping on my side help with haemorrhoids?
Lying on your left side can help reduce the pressure of the uterus on the major pelvic veins, which may improve blood flow and reduce swelling.
Can I prevent haemorrhoids during my next pregnancy?
Focusing on a high-fibre diet, staying hydrated, and doing pelvic floor exercises from early pregnancy can help reduce the risk of recurrence.
Why does progesterone cause constipation?
Progesterone relaxes the smooth muscles of the intestines, which slows down the movement of food and waste through the digestive tract.
Authority Snapshot (E-E-A-T)
This patient education is designed to provide accurate, evidence-based information regarding pregnancy and haemorrhoids for the UK public. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in obstetrics, gynaecology, and general surgery. All information provided is strictly aligned with the clinical standards and quality protocols set by the NHS and the National Institute for Health and Care Excellence (NICE).
