Haemorrhoids, commonly referred to as piles, are a frequent occurrence in the United Kingdom and can often be managed effectively through dietary adjustments and over the counter treatments. While mild cases typically resolve within a few days, certain symptoms or persistent changes in bowel habits require a formal clinical evaluation to ensure an accurate identification of the cause. Understanding the distinction between routine discomfort and clinical indicators that warrant investigation is essential for maintaining gastrointestinal health and ensuring that any underlying conditions are identified and managed according to national health standards.
What We’ll Discuss in This Article
- Indicators for seeking a routine appointment with a healthcare professional
- Clinical red flags associated with rectal bleeding and bowel changes
- The importance of age and medical history in determining risk
- Diagnostic procedures used by clinicians to investigate anal symptoms
- Recognising complications such as thrombosis and strangulation
- The role of pharmacists and General Practitioners in the management pathway
General Indicators for Seeking Medical Advice
You should see a doctor about haemorrhoids if your symptoms do not improve after one week of following healthy lifestyle habits and using over the counter treatments. While many minor flare ups subside once constipation is managed and straining is reduced, persistent symptoms suggest that the haemorrhoids may be of a higher grade or that another factor is contributing to the irritation. A clinical review allows a healthcare professional to assess the severity of the swelling and determine if a referral for non surgical procedures, such as rubber band ligation, is necessary.
In many instances, the initial point of contact for minor anal symptoms in the UK is a community pharmacist. They can provide advice on soothing creams and ointments while screening for symptoms that require a GP consultation. If the itching, soreness, or feeling of fullness remains constant despite these interventions, a formal appointment is the established next step. This ensure that the management plan is tailored to the individual and that the physical cushions in the anal canal are not causing long term structural issues.
Investigating Rectal Bleeding and Bowel Changes
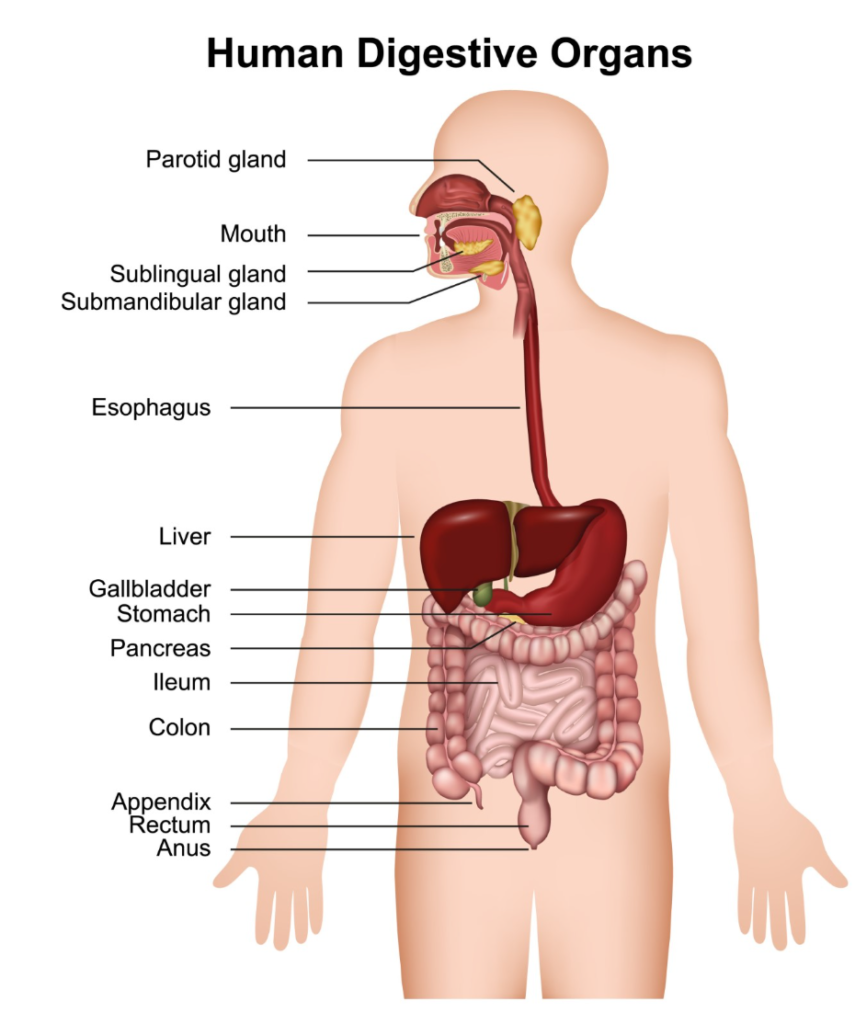
Rectal bleeding is a hallmark sign of haemorrhoids but must always be evaluated by a medical professional to rule out other potential causes within the colon or rectum. Haemorrhoids are swollen veins in the anus and lower rectum, and while they frequently cause bright red blood on the toilet paper, any rectal bleeding should be checked by a GP to confirm the diagnosis. Clinicians use the colour, volume, and frequency of the bleeding to decide on the appropriate investigation pathway.
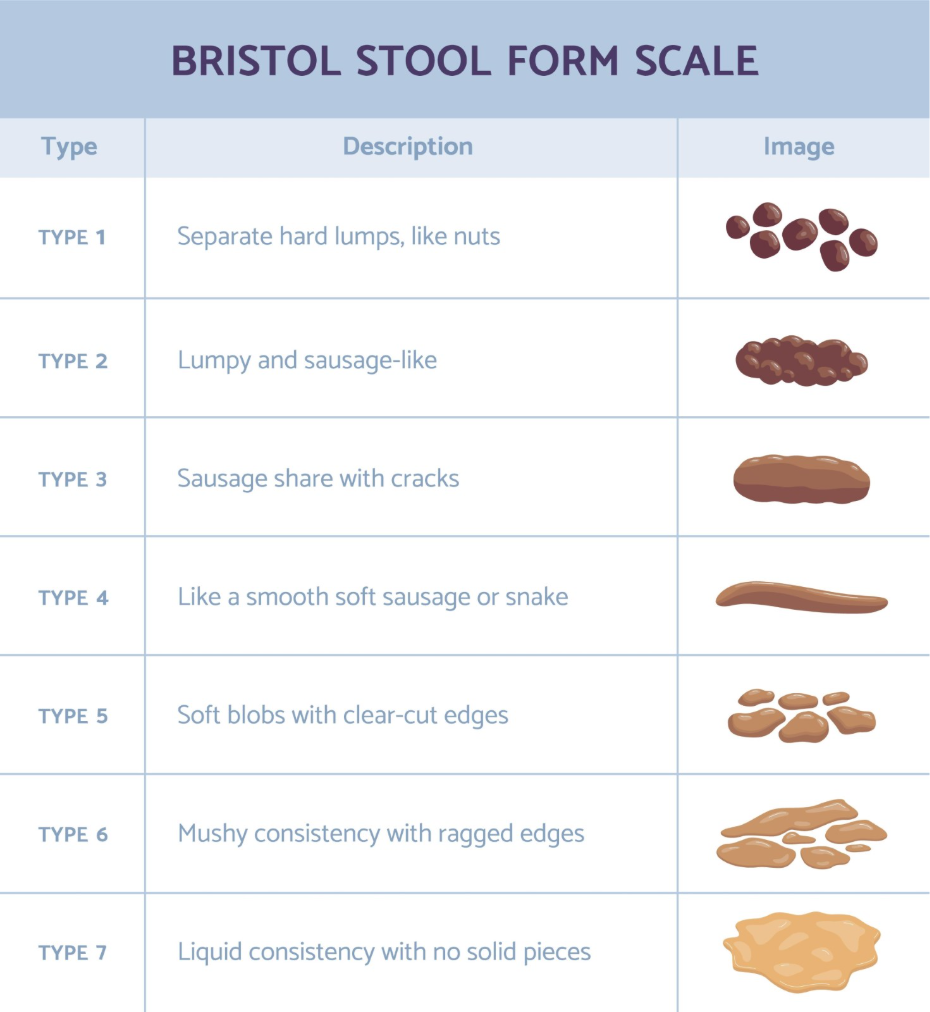
A persistent change in bowel habit that lasts for three weeks or more, such as going to the toilet more often or having looser stools, is a significant clinical indicator that requires investigation alongside haemorrhoid symptoms. The National Institute for Health and Care Excellence provides structured guidelines for the investigation of unexplained changes in bowel habit or rectal bleeding to ensure that organic diseases are excluded effectively. This is particularly important if the blood is dark in colour or mixed within the stool, as this suggests the source may be higher up in the digestive tract than the anal canal.
Recognising Complications and Acute Pain
Severe or sudden pain associated with a lump in the anal area is a clinical indicator that a complication has occurred, such as a thrombosed or strangulated haemorrhoid. A thrombosed haemorrhoid occurs when a blood clot forms inside an external vein, resulting in a hard, bluish lump that is extremely tender to the touch. While not typically an emergency, the intensity of the pain often requires a medical assessment to manage the inflammation or to consider a minor procedure to release the pressure if caught in the early stages.
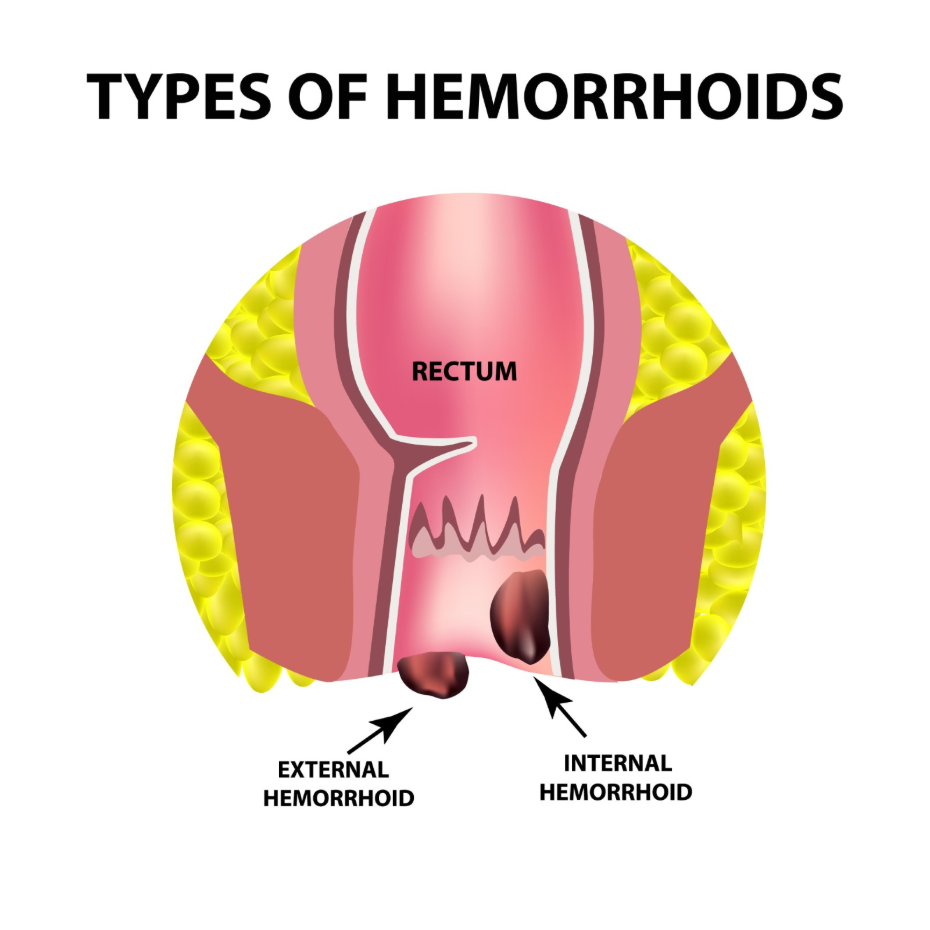
Strangulation happens when an internal haemorrhoid prolapses (protrudes outside the anus) and its blood supply is cut off by the anal sphincter muscles. This can lead to intense pain and tissue damage, requiring urgent clinical review. If a lump cannot be pushed back inside or if the pain prevents normal activities such as sitting or walking, professional advice should be sought promptly. These acute changes represent a shift from a functional nuisance to a clinical complication that needs specific management.
Risk Assessment Based on Age and History
The threshold for medical investigation is often lower for individuals over the age of 40 or those with a family history of gastrointestinal conditions. In the UK, clinicians use age as a primary factor in risk stratification for abdominal and rectal symptoms. Persistent bloating, changes in bowel habits, or new rectal bleeding in older adults are investigated more comprehensively to rule out conditions such as colorectal cancer or inflammatory bowel disease.
If you have close relatives who have been diagnosed with bowel conditions, it is important to share this information with your healthcare provider during an assessment for haemorrhoids. This allows the clinician to apply the appropriate diagnostic protocols and determine if more advanced screening, such as a colonoscopy or a Faecal Immunochemical Test, is required. Persistent or frequent rectal symptoms in adults, particularly those with specific risk factors, should be managed through established NHS diagnostic pathways.
Clinical Diagnostic Procedures
When you see a doctor about haemorrhoids, they will typically follow a systematic approach to confirm the diagnosis and assess the health of the rectum. This begins with a detailed discussion of your symptoms, dietary habits, and any medications you are taking. A physical examination is usually required, which may include a visual inspection of the anal area and a digital rectal examination, where the clinician uses a lubricated, gloved finger to check for internal lumps or abnormalities.
In some cases, a GP may use a small instrument called a proctoscope to look more closely at the lining of the anal canal and the lower rectum. This procedure is brief and allows for the direct visualisation of internal haemorrhoids. If there are concerns about the upper colon, or if the initial tests are inconclusive, a referral for an endoscopic procedure may be made. These standard diagnostic steps are essential for ensuring that the symptoms are truly due to benign haemorrhoids and for excluding other inflammatory or structural issues.
| Symptom Category | Routine Appointment | Prioritised Assessment |
| Bleeding | Bright red on tissue only | Dark, mixed with stool, or heavy |
| Lumps | Soft, comes and goes | Hard, persistent, or very painful |
| Bowel Habit | Occasional constipation | Lasting more than 3 weeks |
| Weight | Stable | Unintentional weight loss |
| Pain | Mild itching or soreness | Severe, constant, or prevents sleep |
Conclusion
Haemorrhoids are often manageable at home, but a medical review is necessary if symptoms persist beyond one week or if they are accompanied by red flag indicators. Bright red bleeding, sudden hard lumps, or a lasting change in bowel habits should always be assessed by a healthcare professional to ensure an accurate diagnosis. Following the established clinical pathways in the UK helps maintain digestive health and provides access to effective treatments if conservative measures fail. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why does the doctor need to perform a rectal exam for piles?
A digital rectal exam allows the clinician to check the health of the rectal lining and feel for internal lumps or other abnormalities that cannot be seen from the outside.
Can a pharmacist help with my haemorrhoids?
Yes, UK pharmacists can provide advice on over the counter treatments and help you decide if your symptoms require a consultation with a GP.
What is the “three week rule” for bowel habits?
NHS guidelines suggest that any change in bowel habits lasting three weeks or more should be reported to a doctor to rule out underlying conditions.
Should I see a doctor if my piles don’t hurt?
Yes, if you have painless rectal bleeding or a prolapsed lump that does not resolve, it is important to have a clinical assessment even if there is no pain.
What is a CA125 test and is it for piles?
A CA125 test is a blood test for ovarian health and is not used for haemorrhoids, but it may be offered if persistent bloating is a primary symptom in women.
Can haemorrhoids be a sign of something more serious?
While haemorrhoids themselves are benign, their symptoms can overlap with other conditions, which is why a professional assessment is essential for new or persistent signs.
How do I prepare for a doctor’s appointment about haemorrhoids?
It is helpful to keep a record of your symptoms, including any triggers, the frequency of bleeding, and any changes in your stool consistency or bowel frequency.
Authority Snapshot (E-E-A-T)
This medical education content is designed to provide accurate, evidence-based information for the UK public regarding the clinical management of haemorrhoids. The material is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in general surgery, internal medicine, and acute care. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
