Anal fissures are a frequent cause of rectal bleeding and often present as bright red blood noticed during or after a bowel movement. While the sight of blood can be concerning, bleeding from a fissure is typically a result of a small tear in the lining of the anal canal. Understanding the characteristics of this bleeding and how it differs from other gastrointestinal issues is important for effective management and for knowing when to seek professional medical advice. By recognising the signs of a fissure, individuals can apply the correct self care measures to support tissue repair and maintain long term digestive health.
What We’ll Discuss in This Article
- The physical characteristics of bleeding caused by an anal fissure
- The anatomical reasons why the anal lining is susceptible to tearing
- Differentiating between fissure bleeding and other conditions like piles
- The impact of stool consistency on the frequency of bleeding episodes
- How muscle spasms in the anal canal can affect healing and bleeding
- Clinical guidelines for when rectal bleeding requires a medical review
Characteristics of Bleeding from an Anal Fissure
Anal fissures cause bleeding that is typically bright red in colour and is most often noticed on the toilet paper or as a small streak on the surface of the stool. An anal fissure is a small tear in the lining of the anus that can cause sharp pain and bright red bleeding during or after a bowel movement. Because the blood comes from a fresh tear at the very end of the digestive tract, it has not been processed or darkened by digestive enzymes, which is why it retains its vivid red appearance. In most cases, the amount of blood is small and does not usually mix with the stool itself.
The timing of the bleeding is closely associated with the act of evacuation. Many patients report a sharp, stinging sensation followed by a small amount of spotting. It is rare for a simple anal fissure to cause heavy bleeding that fills the toilet bowl, but the association between the acute pain and the presence of blood is a key clinical indicator of a tear. Identifying these patterns helps healthcare professionals distinguish a fissure from other potential sources of bleeding higher up in the colon.
Anatomical Reasons for Bleeding
The anal canal is lined with a specialised type of tissue known as anoderm, which is very thin and highly sensitive, making it prone to bleeding if it is overstretched or injured. This tissue contains a high density of sensory nerves and small blood vessels. When a tear occurs, these vessels are exposed and can easily bleed when subjected to the friction of passing waste. The most common location for these tears is the posterior midline, which is the area toward the back of the anal opening.
This region is particularly vulnerable because the blood supply to the posterior midline is naturally less robust than in other parts of the anal canal. When a fissure occurs, the internal anal sphincter muscle often goes into an involuntary spasm to protect the area. This spasm increases the pressure within the anal canal and can further restrict blood flow, which may lead to persistent or recurrent bleeding as the wound struggles to knit back together. The mechanical trauma of passing a hard stool acts as a repetitive injury, preventing the fragile new cells from forming a stable bridge across the tear.
Differentiating Fissure Bleeding from Haemorrhoids
While both anal fissures and haemorrhoids (piles) can cause bright red rectal bleeding, they are distinct conditions with different symptom patterns. Haemorrhoids are swollen blood vessels that often cause painless bleeding, whereas the bleeding from an anal fissure is almost always accompanied by significant, sharp pain. Understanding these differences is essential for ensuring that the correct conservative management is applied.
| Feature | Anal Fissure Bleeding | Haemorrhoid Bleeding (Piles) |
| Pain Level | Sharp, stinging, or burning pain | Often painless (if internal) |
| Timing | During and shortly after pooing | During or after pooing |
| Blood Colour | Bright red | Bright red |
| Blood Location | On the tissue or surface of stool | In the bowl or on the tissue |
| Other Signs | Feeling of a “paper cut” | Feeling of a lump or fullness |
In some instances, a person may experience both conditions simultaneously, particularly if chronic constipation is a factor. However, the management of a fissure focuses primarily on relaxing the anal sphincter muscle and protecting the skin, while haemorrhoid care focuses on reducing vascular pressure. Any instance of rectal bleeding should be professionally assessed to confirm the diagnosis and ensure that symptoms are not related to other gastrointestinal conditions.
Acute versus Chronic Bleeding Patterns
The frequency and nature of the bleeding can indicate whether an anal fissure is in the acute or chronic stage of development. An acute fissure is a new tear that typically heals within six weeks with basic dietary adjustments and high standards of hygiene. During the acute phase, bleeding may occur with every bowel movement, but it usually settles quickly once the stool consistency is improved and straining is avoided.
A chronic fissure is one that has persisted for longer than six weeks and has failed to heal naturally. In these cases, the edges of the tear can become thickened and fibrous, and a small skin tag known as a sentinel pile may develop at the base of the tear. Bleeding from a chronic fissure may be less frequent but can be more difficult to stop because the underlying muscle spasm keeps the wound open. The National Institute for Health and Care Excellence suggests that the first line of management for an anal fissure involves lifestyle changes to ensure stools are soft and easy to pass. Chronic fissures often require specific medicated creams that work by relaxing the anal sphincter muscle to improve blood flow and support permanent healing.
The Impact of Stool Consistency on Bleeding
The consistency of the stool being passed is the most significant factor influencing whether a fissure will bleed and how long it will take to heal. Hard, dry stools require more effort to pass and act as an abrasive force against the anal lining, which can easily re-open a healing tear. Conversely, stools that are very loose or acidic due to diarrhoea can cause chemical irritation and stinging, which also hinders the repair of the tissue.
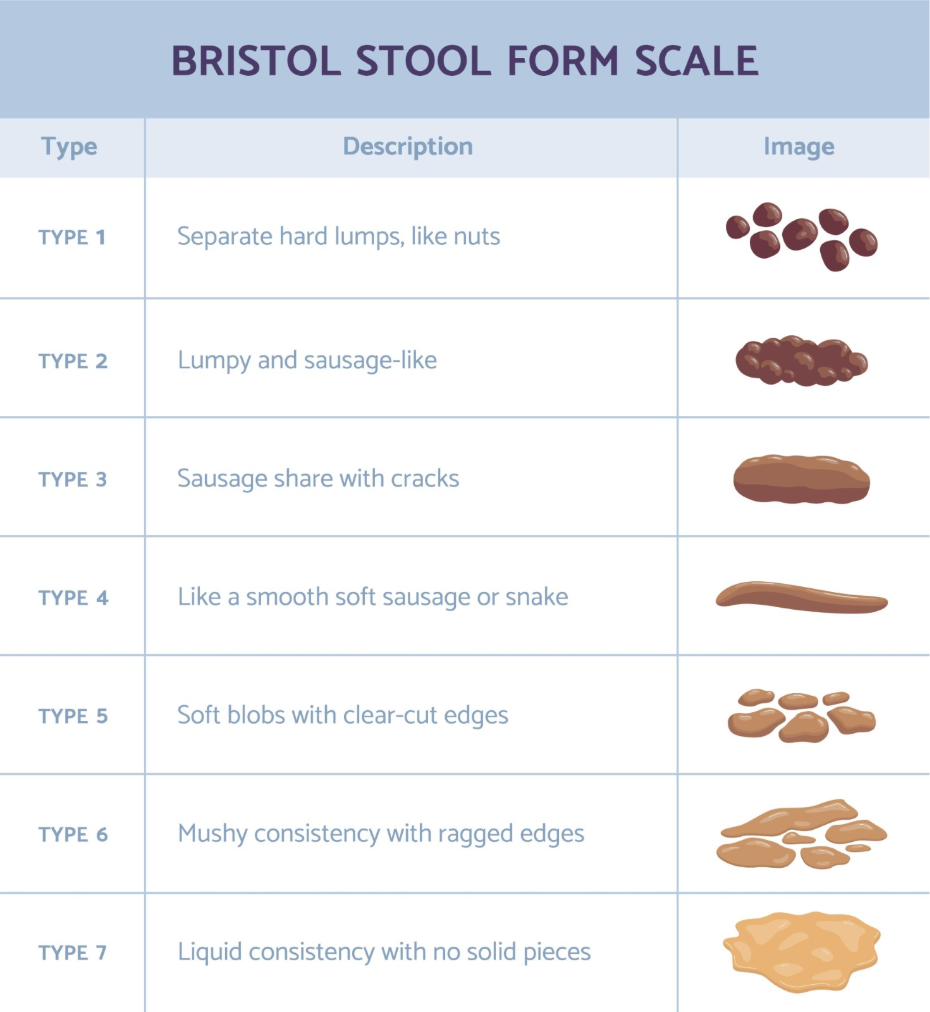
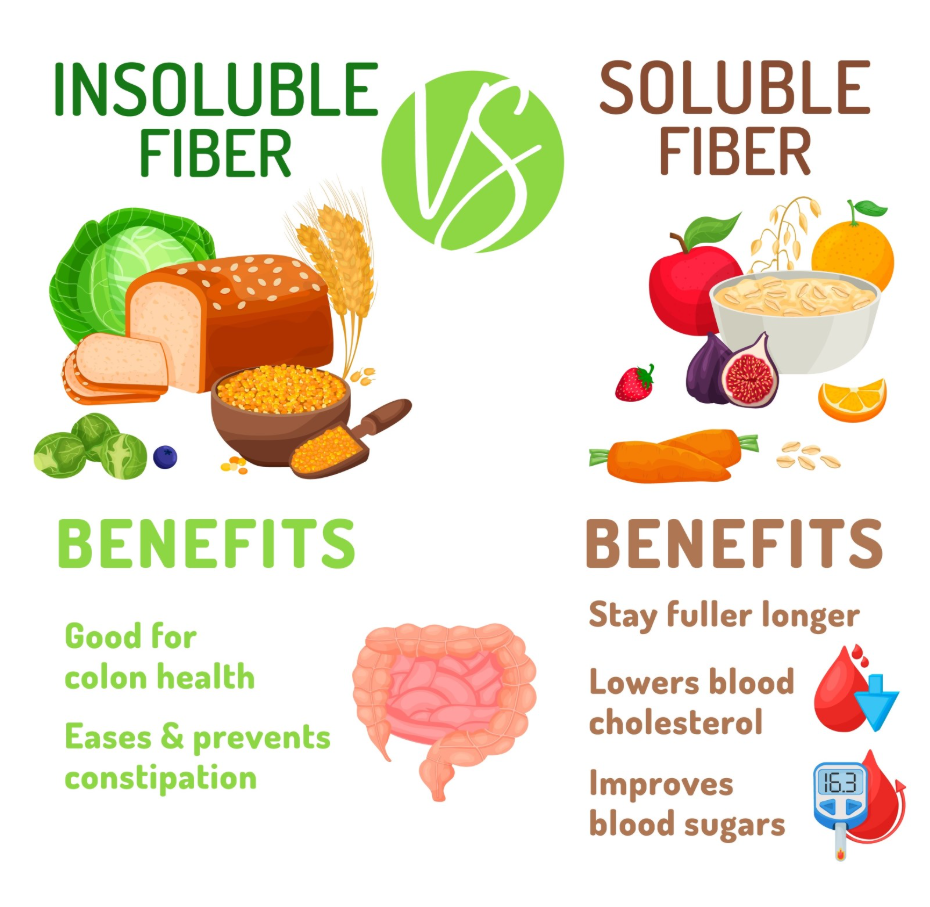
The ideal stool for allowing a fissure to heal is soft and bulky, as this allows the anal canal to open gently without excessive force. Achieving this through a high fibre diet and adequate hydration is the primary recommendation for managing bleeding. Fibre adds weight and volume to the stool, while water ensure that the fibre can move waste through the system effectively. When the stool passes smoothly, the mechanical trauma to the fissure is minimised, reducing the likelihood of fresh bleeding episodes.
Management of Bleeding and Tissue Healing
Managing a bleeding anal fissure involves a combination of softening the stool and using comfort measures to reduce muscle tension and protect the skin. Warm sitz baths, which involve soaking the area in plain warm water for ten to fifteen minutes several times a day, are frequently recommended. The warmth helps the anal muscles to relax, which improves circulation to the tear and can reduce the throbbing pain that often follows a bowel movement.
In addition to warm soaks, maintaining gentle hygiene is vital. The area should be cleaned with plain water and patted dry very gently with a soft towel or dried with a hairdryer on a cool setting. Avoiding the use of scented soaps, alcohol based wipes, or dry, rough toilet paper prevents further chemical and mechanical irritation of the exposed tissue. These simple steps, when combined with a consistent bowel routine, provide the best environment for the anal lining to heal and for the bleeding to stop permanently.
When to Seek a Medical Review for Bleeding
While many anal fissures heal with home care, a medical review is necessary if the bleeding is persistent, heavy, or accompanied by other concerning symptoms. A healthcare professional can perform a gentle visual inspection to confirm the diagnosis and ensure that the bleeding is not related to other issues such as inflammatory bowel disease. In the UK, clinicians follow structured diagnostic pathways to investigate any form of rectal bleeding, especially in individuals over the age of 40.
A clinical assessment should be sought if:
- Rectal bleeding is persistent and does not improve with a high fibre diet
- The blood is dark in colour or mixed within the stool itself
- You experience a persistent change in bowel habits lasting three weeks or more
- You notice a hard lump or swelling in the anal area
- You experience unintentional weight loss or severe abdominal pain
Early intervention for a fissure can prevent it from becoming a chronic condition that requires more complex clinical treatment. A GP can provide access to specific medicated ointments that are more effective than standard over the counter creams for healing a tear.
Conclusion
Anal fissures frequently cause bright red rectal bleeding that is typically associated with a sharp, stinging pain during bowel movements. While the symptoms can be alarming, most cases resolve within a few weeks by focusing on stool softness, hydration, and gentle hygiene. Differentiating a fissure from other causes of bleeding and monitoring for any “red flag” signs is essential for maintaining overall digestive health. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why is the blood from a fissure always bright red?
The blood comes from a fresh tear at the very end of the anal canal, meaning it has not been processed or darkened by the digestive system.
Can an anal fissure cause heavy bleeding?
While most fissures cause only small amounts of spotting, persistent or heavier bleeding should always be evaluated by a healthcare professional.
Will the bleeding stop if I use haemorrhoid cream?
Haemorrhoid creams may soothe the area, but they are not designed to treat the muscle spasms that keep an anal fissure from healing.
How long does it take for a fissure to stop bleeding?
Most acute fissures will stop bleeding within a few days once stools are kept soft and the straining that irritates the tear is avoided.
Can I have a bleeding fissure without any pain?
It is rare for an anal fissure to bleed without pain; painless bleeding is more commonly associated with internal haemorrhoids.
Does a fissure bleed more if I have diarrhoea?
Frequent loose stools can cause chemical irritation and constant wiping, both of which can irritate a tear and cause persistent bleeding.
Can exercise make my fissure bleed?
Gentle exercise like walking is beneficial, but heavy lifting or activities that involve significant straining can increase pelvic pressure and trigger bleeding.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence based information regarding anal fissures and rectal bleeding for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK trained physician with experience in general surgery, emergency care, and clinical education. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
