The intense pain experienced when passing stool with an anal fissure is caused by the mechanical stretching of a tear in the sensitive lining of the anal canal and the subsequent involuntary spasm of the internal anal sphincter muscle. While the tear itself is often small, the anatomical region is highly concentrated with sensory nerves that react acutely to the friction and pressure of waste matter. This discomfort is often described as a sharp, cutting sensation that can transition into a long lasting, dull ache. Understanding the physiological mechanisms of this pain helps in applying the correct conservative management techniques to relax the affected muscles and support the natural healing of the delicate mucosal tissue.
What We’ll Discuss in This Article
- The high concentration of sensory nerves in the anal canal
- Mechanical trauma caused by the passage of stool over a tear
- The role of the internal anal sphincter in causing post-evacuation pain
- How muscle spasms restrict blood flow and delay healing
- The impact of stool consistency on pain intensity
- Clinical guidance for reducing pain during the recovery process
Sensory Nerve Sensitivity in the Anal Canal
Passing stool hurts with a fissure because the anal canal is supplied by a high density of somatic sensory nerves that are extremely sensitive to pain, touch, and stretching. The lining of the lower part of the anal canal, known as the anoderm, is functionally similar to the skin on the fingertips in terms of its ability to detect fine sensations. When a tear occurs in this area, these nerves are exposed and send immediate, sharp pain signals to the brain as soon as the tissue is disturbed.
Unlike the internal rectum, which has limited pain receptors, the anal canal is designed to protect the body by providing acute feedback. An anal fissure is a small tear in the moist, thin tissue that lines the anus, and even a minor injury can cause significant pain due to the sensitive nature of the area. This is why patients often compare the sensation to passing shards of glass; the nerves are reacting to the direct mechanical friction of stool against an open wound.
Mechanical Trauma and Stretching
The act of passing stool requires the anal canal to expand significantly, which directly pulls on the edges of the fissure and prevents the tear from remaining closed. In a healthy state, the anal lining is elastic and accommodates the passage of waste without injury. However, once a fissure is present, every bowel movement acts as a repetitive trauma that re-opens the wound. If the stool is hard or large, the force required to expel it increases the degree of stretching, leading to a spike in pain.
This mechanical stress is a primary reason why fissures can become chronic. The symptoms of an anal fissure often include sharp pain when you go to the toilet and bright red blood on your poo or the toilet paper. Even if the skin has begun to knit together in the hours between bowel movements, the next passage of waste can easily tear the fragile new cells apart. Maintaining soft stools is therefore the most critical factor in reducing the physical trauma that causes this acute pain.
Internal Anal Sphincter Spasms
A significant portion of the pain associated with a fissure is not caused by the tear itself but by the involuntary spasm of the internal anal sphincter muscle that follows a bowel movement. The internal sphincter is a ring of smooth muscle that normally stays contracted to maintain continence. When the sensitive lining is injured, the muscle goes into a defensive spasm to protect the area. This spasm is often felt as a deep, throbbing ache that can last for several hours after leaving the bathroom.
This secondary pain is frequently more distressing for patients than the initial sharp sting because of its duration. The spasm also creates a cycle of discomfort; the muscle tension increases the pressure within the anal canal, which makes the next bowel movement even more difficult to pass. The National Institute for Health and Care Excellence notes that high anal sphincter pressure is a key factor in the development of chronic fissures and the pain that accompanies them. Breaking this cycle through muscle relaxation is a primary goal of clinical treatment.
Restricted Blood Supply and Healing
The muscle spasms that cause pain also restrict the blood supply to the fissure site, which can prevent the tissue from healing and lead to a prolonged period of sensitivity. The blood vessels that supply the anal lining must pass through the sphincter muscles. When these muscles are in a state of high tension or spasm, they compress the vessels, a condition known as ischaemia. This lack of blood flow means the wound does not receive enough oxygen or nutrients to repair itself effectively.
Without adequate blood supply, the edges of the fissure can become thickened and fibrous, and the wound remains “raw” for longer. This explains why the pain remains consistent over many days or weeks. Clinical treatments, such as certain medicated creams, are designed specifically to relax the muscle and restore this vital blood flow. By improving circulation, the internal environment of the anal canal becomes more conducive to tissue repair, eventually reducing the underlying cause of the pain.
Impact of Stool Consistency on Pain Intensity
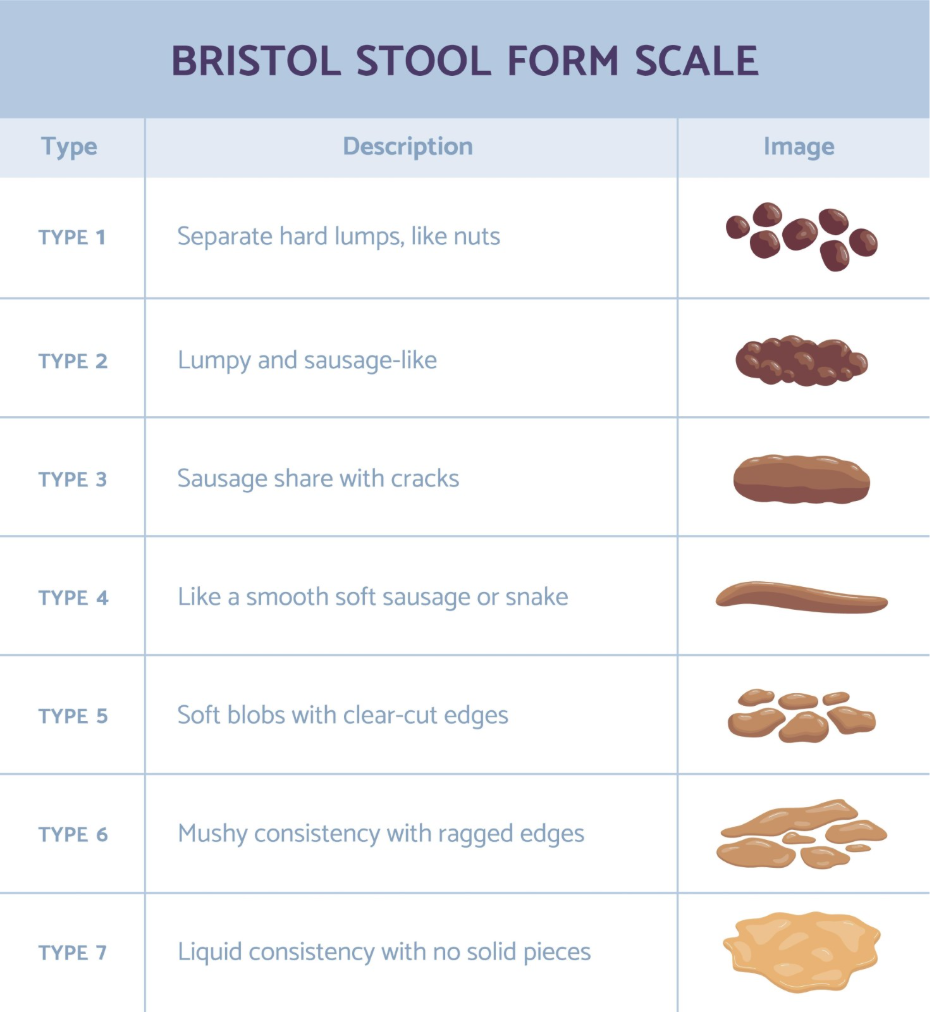
The physical characteristics of the stool being passed determine the level of friction and stretching the fissure is subjected to, directly influencing the intensity of the pain. Hard, dry stools (Type 1 or 2 on the Bristol Stool Form Scale) require more effort to pass and act as an abrasive surface against the tear. Conversely, stools that are too loose or acidic due to diarrhoea can cause chemical irritation and stinging in the open wound.
| Stool Type | Impact on Fissure | Pain Level |
| Hard and Lumpy | Severe stretching and abrasive friction | Very High |
| Soft and Formed | Minimal stretching; passes smoothly | Low to Moderate |
| Liquid/Diarrhoea | Chemical irritation and frequent wiping | High (stinging/burning) |
The ideal stool consistency for a patient with a fissure is soft and bulky. This allows the anal canal to open gently without excessive force and ensures the waste matter slides over the tear with minimal friction. Achieving this through a high-fibre diet and adequate hydration is the most effective way to manage the pain associated with daily bowel movements.
Clinical Strategies to Reduce Passing Pain
Clinical management of the pain involves techniques to relax the anal sphincter and protect the skin from further trauma. Warm sitz baths (soaking the area in plain warm water) are frequently recommended because the warmth helps the internal muscles to relax, which can significantly reduce the post-evacuation throbbing. Additionally, maintaining high standards of gentle hygiene, such as using water instead of dry toilet paper, prevents further mechanical irritation of the tear.
For persistent pain, healthcare professionals may prescribe specific ointments that work by chemically relaxing the anal sphincter muscle. These are distinct from standard haemorrhoid creams and are intended to improve blood flow to the area. If the pain is severe enough to prevent an individual from going to the toilet, or if it does not improve with conservative measures after two weeks, a professional medical review is necessary to ensure the diagnosis is correct and to discuss more advanced management options.
Conclusion
Passing stool hurts with an anal fissure because of the acute sensitivity of the anal nerves and the persistent muscle spasms that follow the passage of waste. The mechanical trauma of stretching the tear combined with a restricted blood supply creates a cycle of pain that can be difficult to break without intervention. By focusing on stool softness, muscle relaxation, and gentle hygiene, most individuals can manage this pain effectively during the healing process. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why does the pain last for hours after I’ve been to the toilet?
The lingering pain is usually caused by the internal anal sphincter muscle going into an involuntary spasm in response to the irritation of the tear.
Can I use numbing creams to stop the pain?
Local anaesthetic creams can provide temporary relief, but they should be used with caution and only as directed to avoid masking worsening symptoms.
Does a fissure ever cause pain when I’m not pooing?
While the sharpest pain is during bowel movements, the muscle spasm can cause a dull ache or throb even when you are not using the toilet.
Is it normal for the pain to be worse in the morning?
Many people find pain is worse with their first bowel movement of the day, especially if the stool has become more compact overnight.
How can I relax the muscle to stop the throbbing?
Soaking in a warm sitz bath for ten to fifteen minutes is one of the most effective ways to relax the anal sphincter and reduce throbbing pain.
Will the pain go away once the bleeding stops?
Not necessarily; while bleeding is a sign of an open tear, the muscle spasms that cause the ache can persist even after the surface has stopped bleeding.
Can exercise make the pain of a fissure worse?
Gentle exercise like walking is beneficial, but activities that involve straining or heavy lifting can increase pelvic pressure and worsen the pain.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information for the UK public regarding the causes of pain from anal fissures. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general surgery, emergency care, and clinical education. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
