Anal intercourse is a recognised cause of anal fissures due to the potential for mechanical trauma to the delicate lining of the anal canal. While fissures are commonly associated with constipation and the passage of hard stools, any activity that results in the overstretching or tearing of the mucosal tissue can lead to a painful split in the skin. Understanding the anatomical risks and the methods for reducing physical friction is a vital part of maintaining sexual health and preventing long term discomfort. If managed correctly with preventative measures and appropriate care, the risk of injury can be minimised, and existing tears can be supported through the natural healing process.
What We’ll Discuss in This Article
- The anatomical vulnerability of the anal canal lining
- How mechanical stretching leads to mucosal tearing during intercourse
- The role of lubrication in preventing physical trauma to the anoderm
- Managing anal sphincter tension and involuntary muscle spasms
- Typical symptoms following an injury to the anal lining
- Clinical advice for managing and healing sexual health-related fissures
Mechanical Trauma and Overstretching
Anal intercourse can cause an anal fissure when the tissue of the anal canal is stretched beyond its elastic limit, resulting in a physical tear. The anal canal is a short tube surrounded by muscular rings known as sphincters, which remain closed to maintain continence. During intercourse, if the canal is not sufficiently relaxed or if the entry is too rapid, the lining can be subjected to excessive force. This force can cause the mucosal tissue to split, usually in a linear fashion.
An anal fissure is a small tear in the lining of the anus, and it can be caused by any trauma to the anal canal, including during anal intercourse. When a tear occurs, it exposes the underlying nerves and, in some cases, the fibres of the internal anal sphincter muscle. The mechanical nature of the injury means that even a single episode of significant stretching can lead to an acute fissure. Because the area is used for the regular passage of waste, an injury caused by intercourse can be easily aggravated, potentially leading to a cycle of pain and difficult healing.
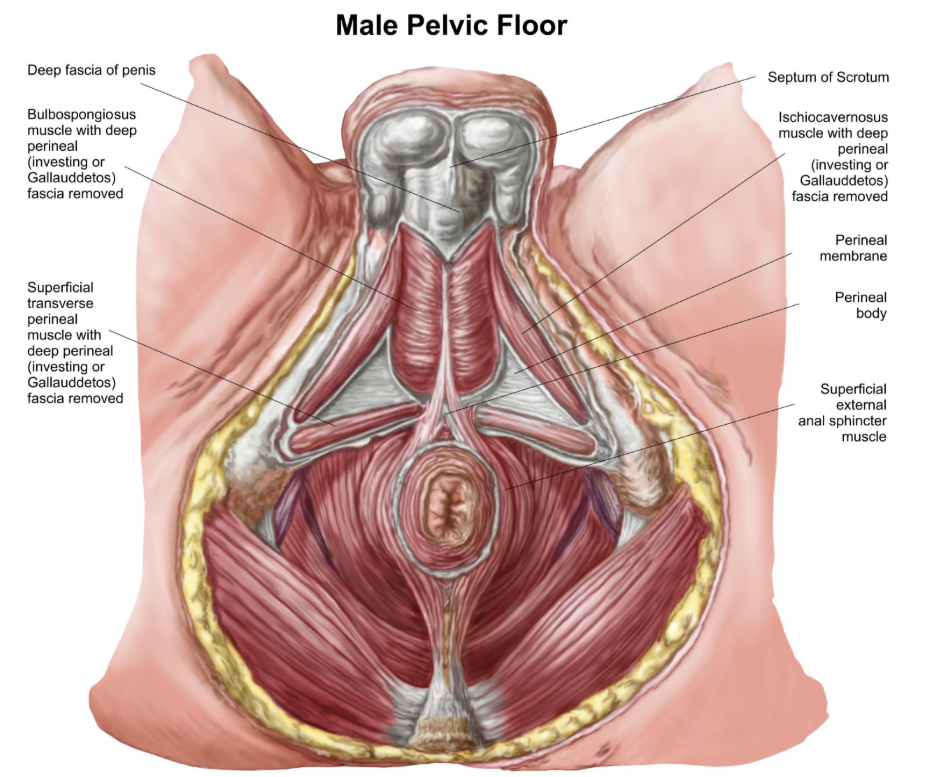
Anatomical Sensitivity of the Anoderm
The lining of the anal canal is highly sensitive and significantly more prone to injury than the skin on other parts of the body. This specific tissue, known as the anoderm, lacks the protective outer layer of keratin found on regular skin, making it moist and fragile. It is densely supplied with sensory nerves that are designed to detect fine changes in pressure and temperature. Because of this high nerve density, even a very small tear can result in intense pain.
The most common site for a fissure is the posterior midline, which is the area toward the back of the anal opening. This region has a naturally lower blood supply compared to the rest of the canal, which makes it less resilient and slower to repair once a tear has occurred. Understanding this anatomical vulnerability is important for anyone engaging in activities that involve the anal canal. The National Institute for Health and Care Excellence notes that anal fissures often result from mechanical injury to the anal mucosa, which can occur during sexual activity. Protecting this delicate tissue requires a cautious approach to physical contact and an awareness of the limitations of its elasticity.
The Importance of Lubrication and Relaxation
Adequate lubrication and relaxation of the anal sphincter muscles are essential for reducing the risk of a tear during anal intercourse. Unlike the vagina, the anal canal does not produce natural lubrication. Without the use of high-quality, water-based or silicone-based lubricants, the friction of intercourse can quickly lead to skin erosion and tearing. The absence of moisture increases the drag on the mucosal lining, causing it to bunch and split under pressure.
The state of the anal sphincter muscles also plays a critical role in preventing injury. The internal anal sphincter is an involuntary muscle that stays contracted; if a person is tense or anxious, this muscle can become even tighter. Attempting intercourse against a constricted sphincter increases the mechanical stress on the anoderm significantly. Taking time to ensure the muscles are relaxed and using sufficient lubrication helps the anal canal to expand more evenly, distributing the pressure and reducing the likelihood of a localised tear forming.
Symptoms and Identification
The symptoms of a fissure caused by intercourse are identical to those caused by other forms of trauma, primarily involving sharp pain and bright red bleeding. Most individuals notice a sharp, stinging, or burning sensation at the moment the injury occurs or during a subsequent bowel movement. This pain is often described as feeling like a paper cut or a shard of glass passing through the area.
Following the initial injury, the internal anal sphincter may go into an involuntary spasm, which can cause a dull, throbbing ache that persists for several hours. Bright red blood may be noticed on the toilet paper or as a streak on the surface of the stool. While these signs are common with fissures, any form of rectal bleeding should be evaluated by a healthcare professional to confirm the source. Recognising these patterns early allows for the prompt application of conservative care, which can prevent an acute tear from becoming a chronic, non-healing wound.
Comparison of Fissure Triggers and Risks
The following table compares the risks associated with different types of mechanical trauma to the anal canal.
| Feature | Constipation-Related Fissure | Intercourse-Related Fissure |
| Primary Mechanism | Internal pressure from hard stool | External mechanical friction and stretching |
| Common Location | Posterior midline (back) | Posterior or anterior midline |
| Lubrication Role | Natural mucus production | Dependent on external lubricants |
| Muscle Factor | Straining against the sphincter | Entry against a tight sphincter |
| Risk of Recurrence | High if diet is not changed | High if preventative measures are not used |
Healing and Management Strategies
Most fissures caused by mechanical trauma will heal within a few weeks if the area is allowed to rest and further irritation is avoided. The primary goal of management is to relax the anal sphincter muscles and ensure that bowel movements remain soft so that they do not re-open the healing tear. Increasing dietary fibre and fluid intake is recommended to prevent constipation, which would otherwise complicate the recovery of a fissure caused by intercourse.
Comfort measures such as warm sitz baths can be highly beneficial. Soaking the area in plain warm water for ten to fifteen minutes several times a day helps the anal muscles to relax and improves blood flow to the site of the injury. It is also advisable to avoid further anal intercourse until the fissure has completely healed, which typically takes between four and six weeks for an acute tear. If the pain is severe or if the fissure does not show signs of improvement, specific medicated creams may be required to break the cycle of muscle spasm and support permanent healing.
Conclusion
Anal intercourse can cause an anal fissure due to the mechanical stress and potential for tearing the sensitive anal lining. Ensuring adequate lubrication and muscle relaxation are the most effective ways to reduce the risk of this injury. Most fissures heal with conservative care, including rest, warm soaks, and maintaining soft stools. If symptoms persist or if you have concerns about rectal bleeding, a medical review is essential. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
How can I tell the difference between a fissure and a haemorrhoid?
Fissures usually cause a sharp, stinging pain during a bowel movement, whereas haemorrhoids are more likely to cause a dull ache or painless bright red bleeding.
Is it safe to have anal sex if I have an existing fissure?
It is recommended to wait until the fissure is fully healed, as further intercourse can re-open the tear and lead to chronic inflammation or infection.
Does using a condom help prevent fissures?
While condoms are essential for preventing infections, they do not prevent fissures; adequate lubrication and relaxation are the primary preventatives for tears.
Can a fissure from intercourse lead to an infection?
Any tear in the skin can potentially become infected, so maintaining high standards of gentle hygiene and allowing the area to rest is important.
How long should I wait before having intercourse again?
Most clinicians suggest waiting at least four to six weeks or until all pain and bleeding have completely resolved before attempting anal intercourse.
Why does it hurt to go to the toilet after a tear from sex?
The passage of stool stretches the anal canal, which pulls on the edges of the tear and irritates the exposed nerves, leading to sharp pain.
Will a fissure heal on its own without medicine?
Many acute fissures heal with simple lifestyle changes like a high-fibre diet and warm baths, but chronic cases may need specific clinical treatments.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information regarding the link between anal intercourse and fissures for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
