Haemorrhoids, frequently referred to as piles, are a common clinical condition involving the swelling of the vascular cushions located within the anal canal. These structures are a normal part of human anatomy, consisting of blood vessels, connective tissue, and smooth muscle, which assist in maintaining bowel continence. Problems arise when these cushions become enlarged, inflamed, or displaced. Understanding the distinction between the internal and external types is essential for appropriate management, as their anatomical origins dictate the types of symptoms a patient may experience and the subsequent treatment pathways required.
What We’ll Discuss in This Article
- The anatomical boundary of the dentate line
- Differences in nerve supply and pain perception
- The four-stage grading system for internal haemorrhoids
- Symptoms and complications unique to external haemorrhoids
- Clinical signs such as prolapse and thrombosis
- Evidence-based management strategies aligned with UK standards
Anatomical Location and the Dentate Line
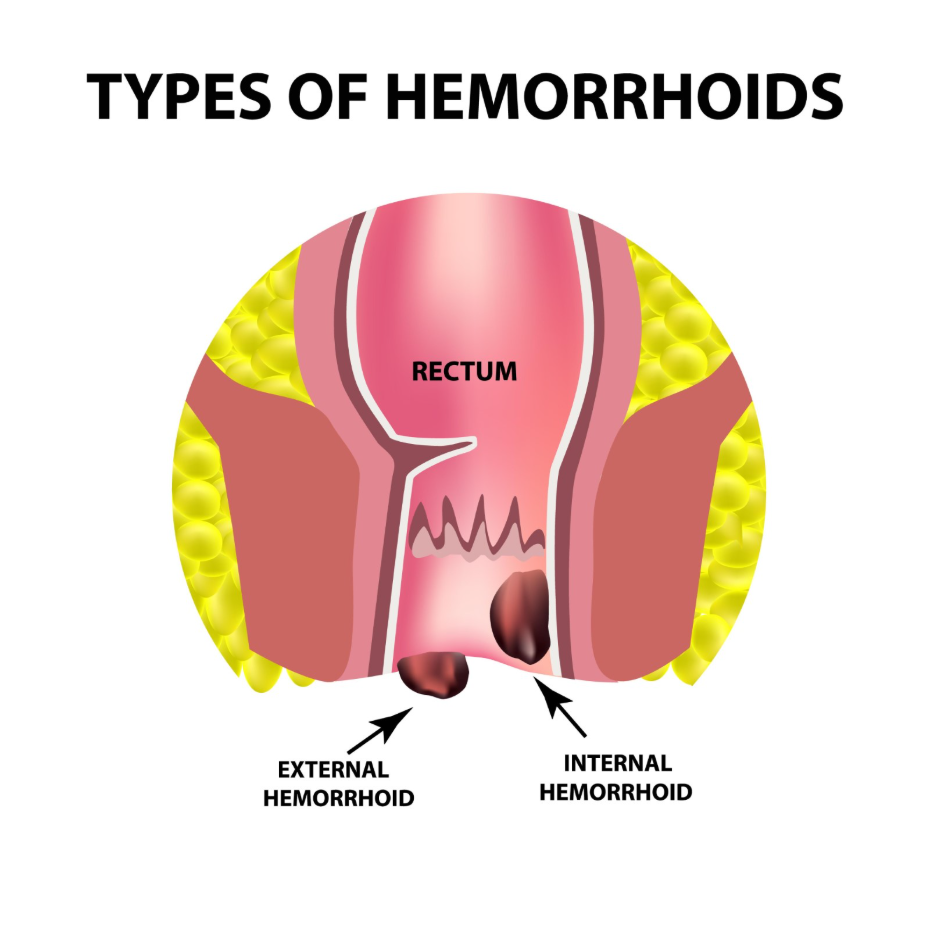
The primary difference between internal and external haemorrhoids is determined by their position relative to the dentate line, a functional landmark in the anal canal. Internal haemorrhoids originate from the upper two-thirds of the anal canal, above this line. They are covered by columnar epithelium, which is a type of tissue similar to the lining of the rest of the digestive tract. Because this area is located deep within the rectum, these swellings are typically not visible from the outside unless they have significantly enlarged and moved downwards.
External haemorrhoids develop in the lower third of the anal canal, below the dentate line. They are covered by anoderm, which is a highly sensitive type of skin. Unlike internal piles, external ones are located under the skin around the anus and are often felt as small lumps. Haemorrhoids, also known as piles, are swellings containing enlarged blood vessels that are found inside or around the bottom. This anatomical distinction is the reason why the two types present with such contrasting sensory experiences.
Nerve Sensitivity and Pain Perception
A fundamental clinical difference between the two types involves the way the body perceives sensation and pain in the affected area. Internal haemorrhoids are supplied by visceral nerves, which are the same type of nerves found in the intestines. These nerves are sensitive to pressure and stretching but do not transmit sharp pain signals. Consequently, internal piles are generally painless, even when they are bleeding or significantly swollen. Many patients may be unaware of their presence until they notice blood after a bowel movement.
In contrast, the area where external haemorrhoids develop is supplied by somatic nerves, similar to the nerves in the skin on the rest of the body. These nerves are highly sensitive to pain, temperature, and touch. This is why external haemorrhoids are frequently associated with significant discomfort, sharp pain, or persistent itching. When an external haemorrhoid becomes irritated or develops a complication, the sensation is usually immediate and localised.
Symptoms and Grading of Internal Haemorrhoids
The most frequent indicator of internal haemorrhoids is bright red, painless rectal bleeding during or after passing stool. Because the tissue is fragile, the passage of waste can cause minor trauma to the surface of the swelling. Internal piles are often classified by a four-stage grading system based on the degree to which they protrude, or prolapse, from the anal canal.
- Grade I: These remain entirely internal and do not protrude from the anal opening.
- Grade II: These protrude during a bowel movement but return inside the rectum spontaneously afterwards.
- Grade III: These protrude and do not return on their own, requiring the patient to manually push them back inside.
- Grade IV: These are permanently prolapsed and cannot be pushed back inside, often leading to mucus discharge and skin irritation.
As internal haemorrhoids reach higher grades, they may cause a sensation of fullness or the feeling that the bowel has not completely emptied. The presence of mucus on the skin from the prolapsed tissue can also lead to secondary itching, known as pruritus ani.
Symptoms and Complications of External Haemorrhoids
External haemorrhoids primarily present as visible or palpable lumps around the anal opening. They may cause persistent itching and discomfort, especially during sitting or physical activity. Because they are covered by skin, they do not bleed as readily as internal piles unless the skin becomes broken or irritated. However, a significant complication associated with this type is the development of a perianal haematoma, or a thrombosed external haemorrhoid.
Thrombosis occurs when a blood clot forms inside the swollen vein. This leads to a sudden increase in pressure and the appearance of a hard, bluish, and extremely painful lump. While the body eventually reabsorbs the clot, it often leaves behind a residual skin tag. The National Institute for Health and Care Excellence provides specific guidelines for the classification and management of haemorrhoidal disease in the United Kingdom. These clinical markers help healthcare professionals determine if a procedure, such as a minor incision to remove a clot, is necessary in the acute phase.
Comparison of Clinical Features
The following table summarises the core differences between the two classifications to help clarify their presentation.
| Feature | Internal Haemorrhoids | External Haemorrhoids |
| Origin | Above the dentate line | Below the dentate line |
| Tissue Covering | Columnar epithelium (mucosa) | Anoderm (highly sensitive skin) |
| Pain Level | Usually painless | Often painful or itchy |
| Primary Symptom | Bright red bleeding | Visible/palpable lumps |
| Prolapse | Possible (Grades I-IV) | Not applicable (always external) |
| Thrombosis | Rare | Common (painful blood clots) |
Management and UK Clinical Standards
The management of both internal and external haemorrhoids begins with conservative measures designed to soften the stool and reduce straining. Increasing dietary fibre to approximately 25 to 30 grams per day and maintaining a fluid intake of roughly two litres are essential steps. These changes help ensure that waste passes through the anal canal with minimal pressure on the vascular cushions.
For symptomatic relief, over-the-counter creams and ointments may be used to reduce inflammation and numb the area temporarily. In the UK, if conservative measures fail, several non-surgical and surgical options are available. Rubber band ligation is a frequent choice for Grade II and III internal haemorrhoids, involving the placement of a small band to cut off the blood supply. For external piles or severe internal ones, surgical removal or stapling may be considered by a specialist. The clinical pathway is determined by the specific type, the degree of prolapse, and the impact on the patient’s quality of life.
Conclusion
The difference between internal and external haemorrhoids is fundamentally anatomical, based on their position relative to the dentate line. Internal piles are often painless and identified by bleeding or prolapse, whereas external piles are characterised by pain, itching, and palpable lumps. Both types are generally manageable through lifestyle modifications and structured clinical interventions. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can you have both internal and external haemorrhoids at the same time?
It is quite common for patients to develop both types simultaneously, which is sometimes referred to as mixed haemorrhoids.
Do internal haemorrhoids always require surgery?
No, most internal haemorrhoids are managed with diet, lifestyle changes, or non-surgical procedures like rubber band ligation.
Why do haemorrhoids itch?
Itching is often caused by mucus discharge from internal piles or skin irritation from the swelling of external piles.
What is a thrombosed haemorrhoid?
This is an external haemorrhoid where a blood clot has formed, causing sudden, intense pain and a hard, bluish lump.
Is blood on the toilet paper always a sign of piles?
While bright red blood is a common sign of haemorrhoids, it can also indicate other conditions, so a clinical assessment is necessary for any rectal bleeding.
Can external haemorrhoids be pushed back in?
No, external haemorrhoids originate outside the rectum and are not designed to be pushed inside; only prolapsed internal haemorrhoids are manually reducible.
Do haemorrhoids turn into cancer?
No, haemorrhoids are swollen veins and do not have the potential to become cancerous, although their symptoms can sometimes mimic those of more serious conditions.
Authority Snapshot (E-E-A-T)
This medical content is designed to provide accurate, evidence-based education for the UK public regarding the clinical presentation of haemorrhoids. The material is produced by a dedicated medical content team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience across internal medicine, general surgery, and acute care. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
