Surgery for haemorrhoids is generally considered a final management option when conservative treatments, lifestyle modifications, and non-surgical clinical procedures have failed to provide adequate relief. While the majority of haemorrhoid cases in the United Kingdom are managed effectively with high-fibre diets and topical treatments, a small proportion of patients with advanced or persistent piles may require surgical intervention. National guidelines prioritise surgery for specific clinical scenarios, such as high-grade prolapse or severe complications, to improve quality of life and resolve chronic symptoms. Understanding the criteria for surgical referral is essential for patients navigating the treatment pathway within the UK health system.
What We’ll Discuss in This Article
- Clinical grading and its role in determining surgical necessity
- Situations where non-surgical treatments have proven ineffective
- The impact of chronic symptoms on the decision for surgery
- Specific complications that warrant an urgent surgical review
- Common surgical procedures performed in the UK
- Post-operative expectations and long-term recovery
Grading of Haemorrhoids and Surgical Thresholds
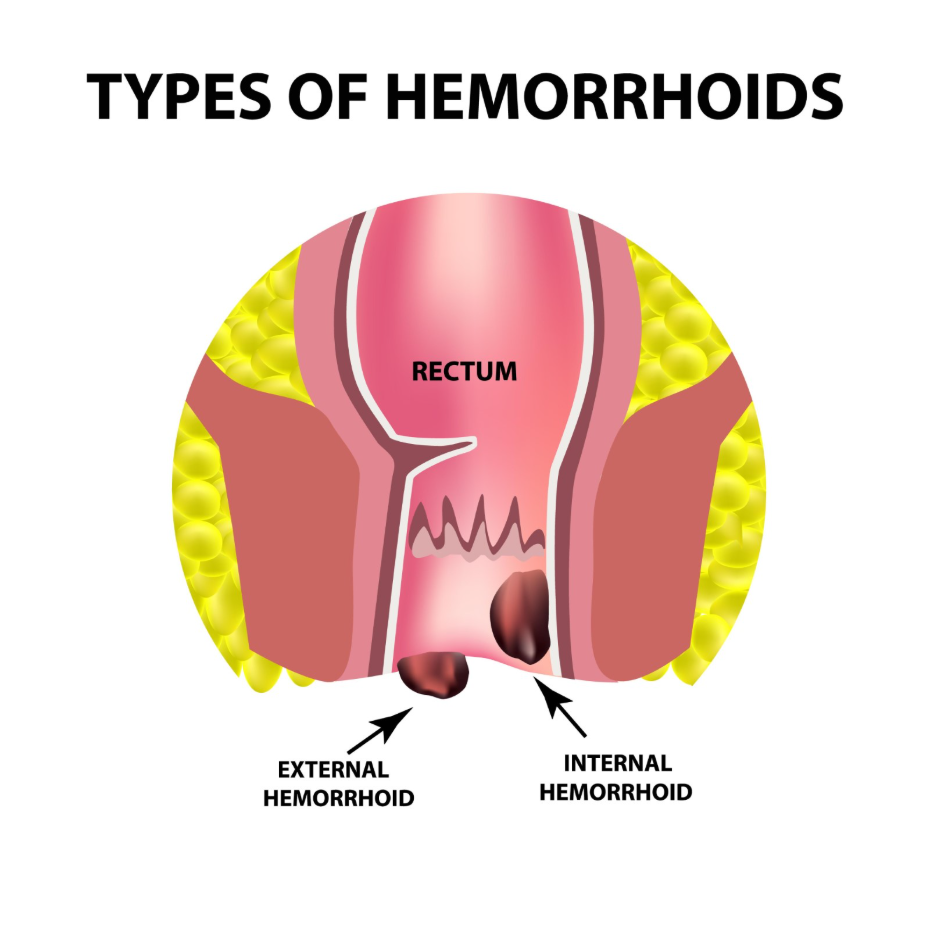
Surgery is most commonly recommended for individuals with grade three or grade four internal haemorrhoids that cause significant daily distress. Haemorrhoids are classified into four grades based on the extent to which the vascular cushions protrude from the anal canal. Grade one and two haemorrhoids, which either remain internal or return spontaneously after a bowel movement, rarely require surgical removal.
In contrast, grade three haemorrhoids require manual replacement by the patient, and grade four haemorrhoids remain permanently prolapsed outside the anus. The National Institute for Health and Care Excellence suggests that surgery should be considered for internal haemorrhoids that fail to respond to non-surgical management or for those with high-grade prolapse. When the connective tissues supporting these vessels have stretched to the point that the tissue cannot stay internal, surgical repositioning or removal becomes the primary method to restore normal anatomy and function.
Failure of Non-Surgical Clinical Procedures
A patient is often referred for surgery when outpatient procedures, such as rubber band ligation or sclerotherapy, have not successfully resolved the symptoms. Non-surgical methods are frequently the first clinical step for internal piles, involving the use of small elastic bands to cut off blood supply or chemical injections to shrink the vessels. While effective for many, some individuals experience a recurrence of symptoms shortly after these procedures.
If a patient undergoes multiple rounds of banding without long-term improvement, a consultant surgeon may determine that the haemorrhoidal tissue is too extensive for outpatient management. Haemorrhoids are swollen veins in the anus and lower rectum, and if simple treatments or clinical procedures like banding do not work, surgery may be necessary. This transition to surgery ensures that the root cause of persistent bleeding, discharge, or discomfort is addressed more permanently through direct excision or arterial ligation.
Chronic Symptoms and Quality of Life
The decision to proceed with surgery is often influenced by the impact of chronic symptoms, such as persistent bleeding and hygiene challenges, on a person’s daily life. Even if haemorrhoids are not classified as grade four, they may be deemed surgical if they cause recurrent, heavy rectal bleeding that could lead to secondary health issues such as anaemia. Similarly, significant mucus discharge associated with prolapsed tissue can cause chronic skin irritation and maceration, which may be difficult to manage with conservative measures alone.
When symptoms interfere with the ability to work, exercise, or maintain personal comfort, the clinical benefits of surgery may outweigh the risks of the procedure. Patients and their clinicians will discuss the frequency of flare-ups and the effectiveness of previous interventions. In the UK, the focus is on providing a long-term solution that reduces the need for repeated courses of topical medications or frequent clinical visits.
Complications Requiring Surgical Review
Certain acute complications, such as strangulated haemorrhoids or severe thrombosis, may warrant an urgent surgical evaluation to prevent further tissue damage. Strangulation occurs when a prolapsed internal haemorrhoid is trapped by the anal sphincter muscles, cutting off its blood supply. This is a painful condition that can lead to tissue death (necrosis) if not managed promptly.
While most thrombosed external haemorrhoids resolve with time as the body reabsorbs the clot, some cases involve such extreme pain or extensive swelling that a minor surgical procedure is needed to release the pressure. A thrombosed haemorrhoid can cause a sudden, severe pain and a hard lump around the anus that is very tender to the touch, and in some cases, surgical intervention is required to provide relief. These scenarios represent a shift from elective management to a clinical necessity to protect the integrity of the anal canal.
Overview of Common Surgical Procedures
Several surgical techniques are utilised in the UK to treat haemorrhoids, each with specific indications based on the patient’s symptoms and the grade of the piles. A traditional haemorrhoidectomy involves the surgical excision of the haemorrhoidal tissue and is often reserved for the most severe cases. While it has a high success rate for preventing recurrence, it usually requires a longer recovery period.
| Procedure | Description | Typical Recovery |
| Haemorrhoidectomy | Surgical removal of the haemorrhoid tissue | 2 to 4 weeks |
| Stapled Haemorrhoidopexy | Repositioning and stapling of prolapsed tissue | 1 to 2 weeks |
| Haemorrhoidal Artery Ligation | Tying off the blood supply using ultrasound | 1 week |
Stapled haemorrhoidopexy and haemorrhoidal artery ligation are alternative techniques that often involve less post-operative pain. Stapling focuses on repositioning the tissue higher in the rectum, while artery ligation uses ultrasound to precisely locate and tie off the specific vessels supplying the piles. A consultant surgeon will help determine which method is most appropriate based on whether the primary issue is bleeding, prolapse, or external swelling.
Post-Operative Expectations and Long-Term Care
Recovery from haemorrhoid surgery requires a commitment to maintaining soft stools and healthy bowel habits to ensure the surgical site heals correctly and to prevent new piles from forming. Patients are typically advised to follow a high-fibre diet and increase fluid intake immediately after the procedure. Straining during bowel movements must be avoided, as this can place stress on the internal sutures or the healing tissue.
Most patients can return to light activities within a week or two, though complete healing of a haemorrhoidectomy site may take longer. Follow-up appointments are usually scheduled to monitor the recovery process and ensure that the anal sphincter is functioning normally. The long-term success of any surgical intervention for haemorrhoids is heavily dependent on the patient’s adherence to the lifestyle modifications that reduce pelvic venous pressure.
Conclusion
Surgery for haemorrhoids is generally reserved for high-grade cases, failed non-surgical treatments, or acute complications like strangulation. While the prospect of surgery can be daunting, modern techniques in the UK aim to resolve symptoms effectively while minimising recovery time. Most individuals will continue to manage their condition with conservative measures, but for those with chronic, severe piles, surgery provides a definitive clinical pathway. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is haemorrhoid surgery painful?
Post-operative discomfort is common, especially with traditional excision, but it is managed with prescribed analgesia and stool softeners.
Will my haemorrhoids come back after surgery?
While surgery is highly effective, new haemorrhoids can develop if the underlying causes, such as constipation and straining, are not addressed.
How long will I be off work after surgery?
Depending on the type of procedure and the nature of your job, you may need between one and four weeks for a full recovery.
Are there risks associated with haemorrhoid surgery?
As with any surgery, there are risks such as infection or temporary difficulty passing urine, which your surgeon will discuss with you.
Can I have surgery if I am pregnant?
Surgery is usually avoided during pregnancy as haemorrhoids often resolve after birth; management focuses on conservative comfort measures.
What is the difference between banding and surgery?
Banding is a minor outpatient procedure for internal piles, while surgery is a more comprehensive treatment performed in an operating theatre.
Do I need a general anaesthetic for piles surgery?
Most haemorrhoid surgeries are performed under general anaesthetic or regional anaesthesia (like a spinal block) to ensure patient comfort.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information regarding the criteria for haemorrhoid surgery for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in general surgery and internal medicine. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
