Anal fissures are primarily caused by physical trauma or excessive stretching of the delicate lining of the anal canal, leading to a small tear in the mucosal tissue. While the most common trigger is the passage of hard or large stools associated with constipation, various other factors involving pressure, inflammation, or restricted blood flow can also contribute to the development of a fissure. Understanding the biological and mechanical reasons why these tears occur is essential for effective management and the prevention of future occurrences, ensuring that the sensitive anal lining remains healthy and intact.
What We’ll Discuss in This Article
- The mechanical impact of constipation and hard stools
- How persistent diarrhoea can lead to chemical and physical irritation
- The role of pregnancy and childbirth in increasing pelvic strain
- How high anal sphincter muscle tone prevents natural healing
- Secondary causes related to inflammatory bowel conditions
- Lifestyle factors that influence the risk of developing a tear
Constipation and Mechanical Trauma
The most frequent cause of an anal fissure is the mechanical trauma caused by the passage of hard, dry, or unusually large stools. When waste material sits in the colon for too long, the body reabsorbs excessive amounts of water, resulting in a stool that is difficult to expel. As this stool passes through the anal canal, it can overstretch the lining beyond its elastic limit, causing a linear tear to form, typically at the posterior midline of the anus.
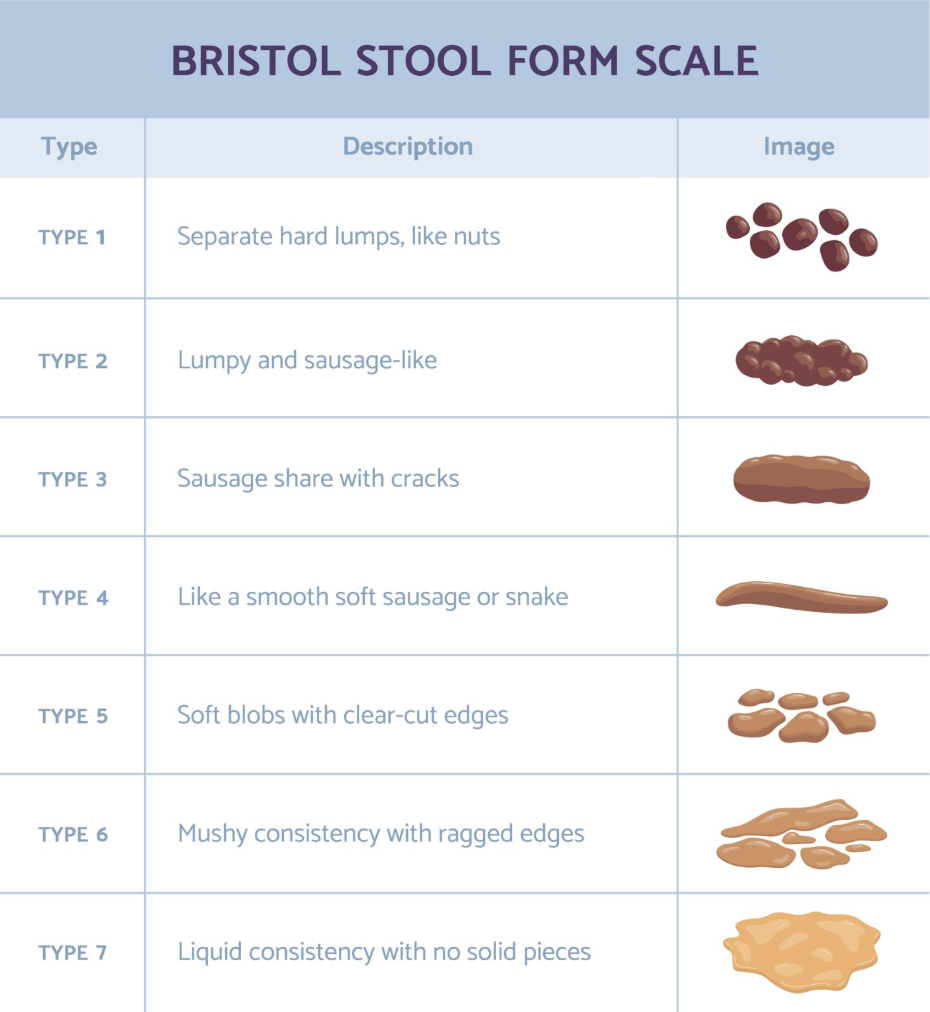
Straining during a bowel movement further compounds this risk by increasing the internal pressure against the anal walls. An anal fissure is a small tear in the lining of the last part of the large intestine (the anal canal), and it is most commonly caused by constipation when a person passes a large or hard stool. This direct physical injury is often immediate, resulting in the sharp, stinging pain that many individuals report at the moment of evacuation. Because the anal lining is thin and sensitive, even a single episode of significant straining can be enough to initiate a fissure.
Persistent Diarrhoea and Chemical Irritation
While constipation is the leading cause, frequent or persistent diarrhoea can also lead to the development of an anal fissure due to constant irritation and chemical inflammation. Frequent loose stools involve multiple bowel movements in a short period, which can cause the anal skin to become sore, macerated, and fragile. The liquid waste often contains higher concentrations of digestive enzymes and bile salts which can irritate the mucosal lining, making it more susceptible to tearing.
Furthermore, the act of frequent wiping during a bout of diarrhoea can cause micro-trauma to the perianal area, further weakening the tissue. When the skin is already inflamed and damp, it loses its structural integrity, allowing even minor movements or the next bowel movement to create a split in the lining. Managing the underlying cause of the diarrhoea is a key part of allowing the anal canal to rest and heal from this type of cumulative irritation.
Pregnancy and Childbirth
Pregnancy and childbirth are significant risk factors for the development of anal fissures due to the combination of hormonal changes and physical pressure on the pelvic floor. During pregnancy, the hormone progesterone relaxes the smooth muscles of the digestive tract, which often leads to slower gut transit times and constipation. As the pregnancy progresses, the increasing weight of the uterus puts direct pressure on the rectum and anal canal, making the tissues more congested and less flexible.
The intense physical strain during the second stage of labour can also cause a tear in the anal lining. The pressure exerted during pushing is substantial and can result in mechanical injury to the anal canal, similar to how it can cause external haemorrhoids. Anal fissures are common in pregnant women and those who have recently given birth because of the strain placed on the area. Postpartum fissures are often managed conservatively, focusing on soft stools and gentle hygiene while the pelvic tissues recover from the trauma of delivery.
High Anal Sphincter Tone and Spasms
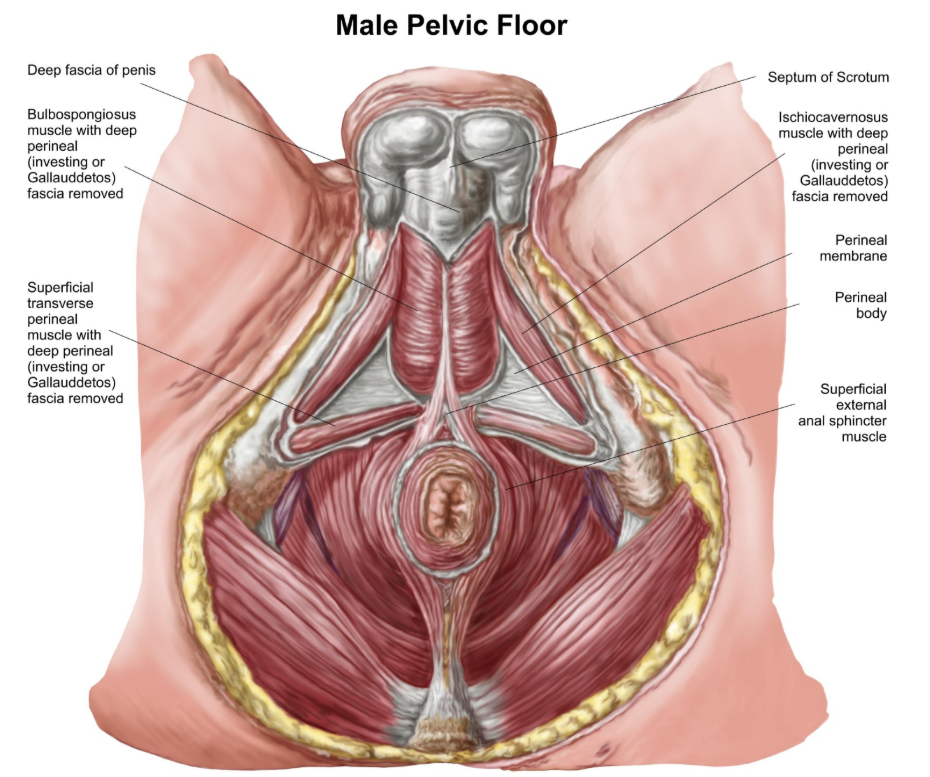
A significant factor in the development of chronic anal fissures is an abnormally high resting pressure in the internal anal sphincter muscle. The anal sphincter is a ring of muscle that stays closed to maintain continence; however, if this muscle is too tight or prone to spasms, it can restrict blood flow to the lining of the anal canal. When blood flow is limited, the mucosal tissue becomes less resilient and more likely to tear during a bowel movement.
Once a tear has occurred, the pain of passing stool can trigger further muscle spasms. This creates a cycle where the spasm increases the pain, and the reduced blood flow prevents the fissure from knitting back together. This physiological environment is often what transforms an acute, fresh tear into a chronic, non-healing wound. The National Institute for Health and Care Excellence provides clinical pathways for treating fissures that involve using medications to relax the anal sphincter muscle and improve local circulation.
Underlying Inflammatory Conditions
In some cases, an anal fissure may be a secondary symptom of an underlying inflammatory condition of the gastrointestinal tract, such as Crohn’s disease or Ulcerative Colitis. These conditions cause chronic inflammation of the digestive lining, which can make the tissue throughout the bowel, including the anal canal, extremely fragile and prone to ulceration or splitting. Fissures associated with these conditions may appear in unusual locations around the anus, rather than the typical midline position.
When a fissure is caused by an inflammatory condition, it often requires a different management approach that focuses on treating the systemic inflammation. Clinicians may look for other symptoms, such as persistent abdominal pain, weight loss, or mucus in the stool, to determine if the fissure is a primary mechanical injury or a sign of a broader health issue. Identifying these cases is essential for ensuring that the patient receives the correct specialist care for their digestive health.
Comparison of Common Fissure Causes
| Cause | Primary Mechanism | Typical Presentation |
| Constipation | Mechanical overstretching | Sharp pain during hard stool |
| Diarrhoea | Chemical irritation and frequent wiping | Burning and soreness |
| Childbirth | Acute pressure and strain | Develops shortly after delivery |
| Sphincter Spasm | Reduced blood flow | Pain that lasts for hours after poo |
| Inflammatory Bowel | Chronic mucosal inflammation | Recurrent or multiple tears |
Lifestyle and Preventative Factors
Certain lifestyle habits can influence the risk of developing the conditions that lead to anal fissures. A diet low in fibre and inadequate fluid intake are the most significant contributors to the constipation that triggers mechanical tears. Fibre adds bulk and retains water in the stool, ensuring it remains soft and passes easily. Without enough water, fibre can actually contribute to harder stools, so both must be managed together.
Sedentary lifestyles can also impact gut motility, making constipation more likely. Conversely, responding immediately to the urge to pass a stool can prevent waste from becoming dry and hard in the rectum. By adopting healthy bowel habits and a balanced diet, individuals can significantly lower the internal and external pressures that cause the anal lining to fail.
Conclusion
Anal fissures are primarily caused by the mechanical stress of constipation and straining, though diarrhoea, pregnancy, and high muscle tone also play significant roles. These factors lead to a tear in the sensitive lining of the anal canal, which can become chronic if muscle spasms restrict the blood flow necessary for healing. While most cases are related to temporary digestive issues, understanding the cause is vital for applying the correct management strategy. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can spicy food cause an anal fissure?
Spicy food does not cause a tear, but it can cause significant stinging and irritation to an existing fissure during a bowel movement.
Why did my fissure appear suddenly?
Most fissures occur acutely following a single episode of passing a particularly hard or large stool that overstretches the anal lining.
Are some people more prone to fissures than others?
Those with chronic constipation, high anal muscle tone, or certain inflammatory conditions are at a higher risk of developing tears.
Can anal sex cause a fissure?
Any form of trauma or significant stretching to the anal canal, including anal intercourse, can lead to a tear in the lining.
Does age affect the risk of getting a fissure?
Fissures can occur at any age, including in infants who experience constipation, but they are most common in young and middle-aged adults.
Why does it hurt more after the bowel movement?
The initial pain is from the tear itself, but the lingering pain is caused by the internal anal sphincter muscle going into a spasm.
How can I prevent a fissure from coming back?
The most effective prevention is maintaining soft stools through a high-fibre diet, staying hydrated, and avoiding straining on the toilet.
Authority Snapshot (E-E-A-T)
This medical education content is designed to provide accurate, evidence-based information for the UK public regarding the causes of anal fissures. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
