An anal fissure is considered chronic when it fails to heal within six weeks, often entering a cycle where physiological factors prevent the natural repair of the torn tissue. While many acute fissures resolve quickly with increased fibre and hydration, chronic cases are characterised by structural changes and persistent muscle tension that restricts blood flow to the injury site. Understanding why certain tears persist allows individuals to identify the signs of a non-healing wound and seek the appropriate clinical interventions to break the cycle of pain and spasm.
What We’ll Discuss in This Article
- The distinction between acute and chronic anal fissures
- The role of internal anal sphincter spasm in preventing healing
- How restricted blood supply (ischaemia) impacts tissue repair
- Physical changes such as sentinel piles and hypertrophied papillae
- The impact of persistent constipation and bowel habits
- Clinical management strategies for chronic anal fissures
Defining the Chronic Anal Fissure
An anal fissure becomes chronic when the initial tear remains open for longer than six weeks, often showing physical signs of long term inflammation and limited healing. In the acute stage, a fissure looks like a simple, shallow tear in the lining of the anal canal. However, as it enters the chronic phase, the edges of the tear often become thickened and raised, and the base of the wound may expose the underlying fibres of the internal anal sphincter muscle.
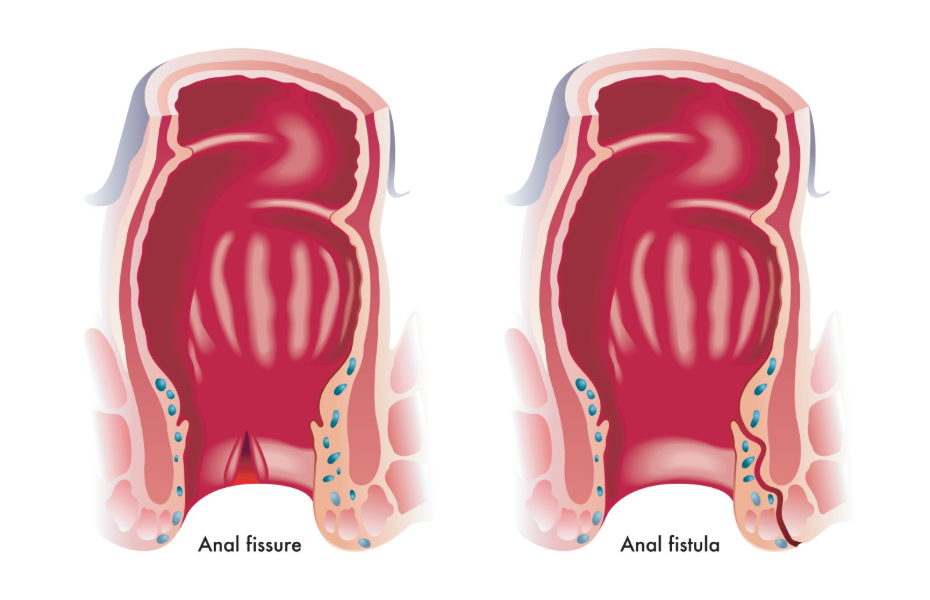
Chronic fissures are frequently associated with secondary physical features that develop as the body attempts to protect the injured area. These may include a small skin tag at the base of the tear, known as a sentinel pile, or a swollen node at the top of the fissure called a hypertrophied papilla. An anal fissure is a small tear in the lining of the anus, and it is classified as chronic if it has not healed after six weeks of conservative treatment. These structural changes indicate that the body is struggling to knit the tissue back together, often requiring more intensive management than a fresh tear.
The Cycle of Sphincter Spasm and Pain
The primary reason a fissure becomes chronic is the development of a cycle involving intense pain and involuntary spasms of the internal anal sphincter muscle. When a tear occurs, the exposure of the sensitive anal lining causes the sphincter muscle to contract sharply to protect the area. This spasm is often felt by the patient as a dull, throbbing ache that persists for several hours after a bowel movement has passed.
The muscle spasm creates a significant problem for healing because it increases the pressure within the anal canal. This high resting pressure makes the act of passing the next stool even more difficult and painful, leading to further injury. The National Institute for Health and Care Excellence provides guidelines for managing chronic fissures, focusing on treatments that relax the anal sphincter to break this cycle of spasm and pain. Without intervention to relax the muscle, the fissure is repeatedly pulled apart, preventing the delicate new skin cells from forming a stable bridge across the gap.
Restricted Blood Supply and Ischaemia
Chronic fissures often persist because the high pressure from muscle spasms restricts the blood supply to the anal lining, a condition known as ischaemia. The blood vessels that supply the posterior midline of the anal canal, where most fissures occur, are already relatively sparse compared to other areas. When the internal anal sphincter muscle is in a state of constant contraction or spasm, it further compresses these small vessels, significantly reducing the amount of oxygen and nutrients reaching the wound.
Adequate blood flow is essential for any wound to heal, as it brings the necessary cells to repair the tissue and fight potential infection. In the case of a chronic fissure, the lack of blood flow creates a “non-healing” environment. The tissue becomes ischaemic, meaning it is starved of the resources it needs to recover. This is why many clinical treatments for chronic fissures involve medications designed specifically to improve local circulation by relaxing the smooth muscle of the anal canal.
Physical Structural Changes Over Time
As a fissure remains unhealed for weeks or months, the body undergoes specific structural changes that can further hinder the healing process. The sentinel pile, or skin tag, that often forms at the external end of the fissure can trap bacteria and moisture, leading to persistent irritation. Similarly, the edges of the tear can become fibrous and “calloused,” making it much harder for the tissue to eventually fuse back together naturally.
These changes are often a sign that the fissure has become deep enough to reach the circular fibres of the internal sphincter. Once the muscle fibres are exposed at the base of the wound, the body’s inflammatory response is heightened. The presence of these structural markers often helps clinicians distinguish between a simple acute tear and a chronic condition that may require specialised ointments or, in some cases, surgical review to reset the healing process.
Impact of Persistent Constipation
Continuing to experience constipation or passing hard stools is a major factor that prevents an acute fissure from healing and turns it into a chronic issue. Every time a hard stool is passed, it mechanically stretches the anal canal and re-opens any healing that may have occurred since the last bowel movement. This repeated trauma ensures that the wound remains fresh and the muscle stays in a state of high tension.
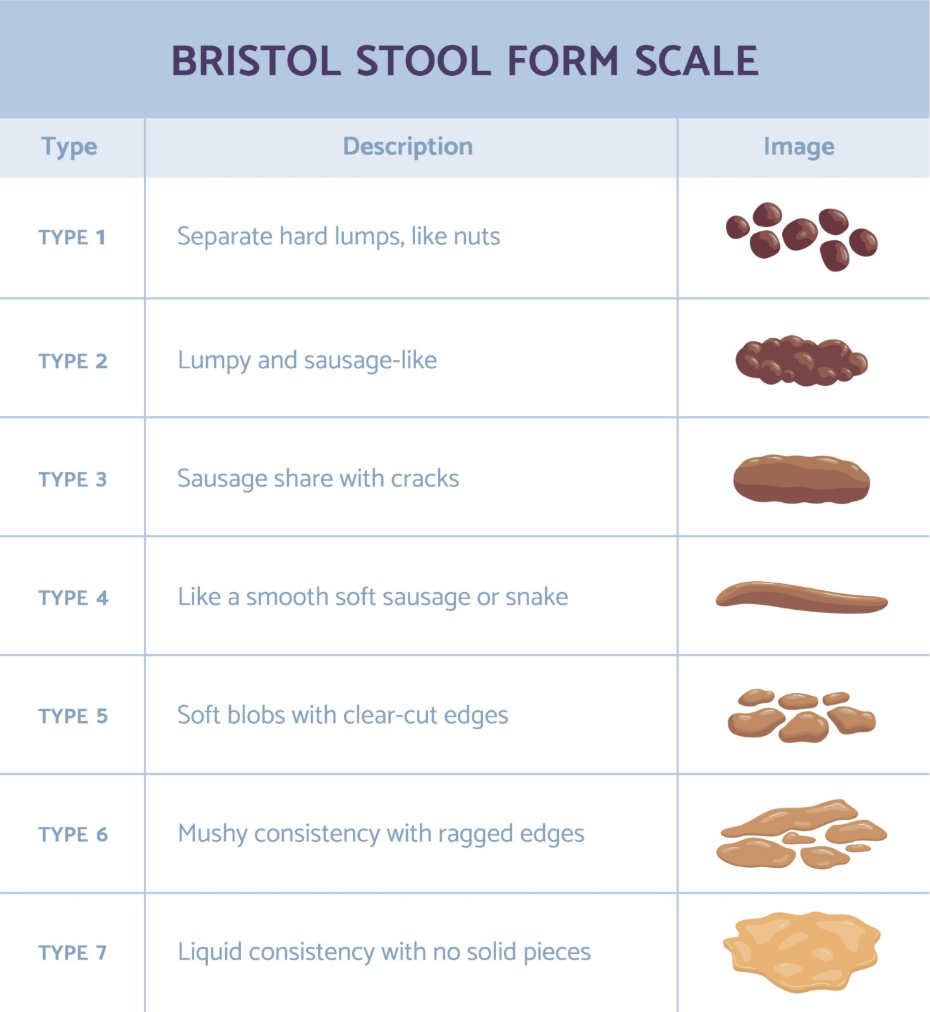
Managing stool consistency is the most vital part of supporting the healing of both acute and chronic fissures. Keeping your poo soft by eating plenty of fibre and drinking enough fluids is the most important step in allowing an anal fissure to heal and preventing it from becoming chronic. If a person does not address the underlying digestive transit issues, even the most effective medications to relax the muscle may fail, as the mechanical injury is simply repeated too frequently for the skin to remain intact.
Differences Between Acute and Chronic Fissures
| Feature | Acute Anal Fissure | Chronic Anal Fissure |
| Duration | Under 6 weeks | Over 6 weeks |
| Appearance | Fresh, shallow “paper cut” | Deep tear with thickened edges |
| Muscle Exposure | Rare | Internal sphincter may be visible |
| Associated Lumps | None | Sentinel pile or papilla often present |
| Healing | Resolves with lifestyle changes | Often requires medicated muscle relaxants |
When to Seek Clinical Intervention
If an anal fissure has not shown significant improvement within a few weeks, or if the pain is becoming increasingly difficult to manage, a professional medical review is necessary. In the UK, GPs follow structured protocols to manage chronic fissures, which often involve prescribing specific creams that work by relaxing the anal sphincter muscle and improving blood flow. These treatments are distinct from standard haemorrhoid creams and are specifically designed for the unique environment of a non-healing tear.
Professional advice is required if:
- The pain is so severe it prevents you from passing a bowel movement
- Rectal bleeding is persistent, heavy, or dark in colour
- The symptoms have persisted for longer than six weeks
- You notice a hard or enlarging lump near the site of the tear
- You experience unintentional weight loss or persistent abdominal pain
Clinicians will assess the area to confirm the diagnosis and ensure that the symptoms are not related to other conditions, such as inflammatory bowel disease. For chronic fissures that remain resistant to topical medications, a referral to a specialist may be made to discuss other options for reducing muscle tension and encouraging permanent healing.
Conclusion
Anal fissures become chronic when a cycle of intense pain and muscle spasm restricts the blood supply needed for tissue repair. This non-healing state is often compounded by persistent constipation and physical changes like skin tags that develop over time. While acute tears often resolve with simple self-care, chronic cases usually require clinical intervention to relax the anal sphincter and restore circulation. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why does my fissure hurt more than it did at the start?
Chronic fissures often hurt more because the muscle spasm becomes more frequent and intense as the wound deepens and exposes more nerves.
Will a chronic fissure ever heal without surgery?
Many chronic fissures heal successfully with specialised medicated creams that relax the anal muscle, though it takes patience and consistent bowel management.
What is a sentinel pile?
A sentinel pile is a small skin tag that forms at the base of a chronic fissure due to long term inflammation and the body’s attempt to protect the area.
Can I use haemorrhoid cream for a chronic fissure?
Haemorrhoid creams are generally not effective for chronic fissures because they do not address the primary issue of muscle spasm and restricted blood flow.
Why is blood flow so important for healing?
Blood carries the oxygen and nutrients needed for skin cells to grow; without it, the tissue remains weak and cannot knit back together.
Can a fissure be chronic if it only hurts occasionally?
Yes, some chronic fissures may have periods of less pain, but if the physical tear remains open for over six weeks, it is still classified as chronic.
What is the best way to prevent a fissure from becoming chronic?
The most effective way is to immediately treat any constipation with fibre and water while using warm soaks to keep the anal muscles relaxed.
Authority Snapshot (E-E-A-T)
This medical education content provides evidence-based information regarding chronic anal fissures for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general surgery, emergency care, and clinical education. All information provided is strictly aligned with the clinical standards and diagnostic protocols provided by the NHS and the National Institute for Health and Care Excellence (NICE).
